Review Article | Volume 2 - Issue 3 | Article DOI :
Download PDF
Alexey Larionov, Peter Yotovski and Luis Filgueira*
University of Fribourg, Faculty of Science and Medicine, Switzerland
Corresponding Author:
Luis Filgueira, University of Fribourg, Faculty of Science and Medicine,1 Albert Gockel, CH-1700 Fribourg, Switzerland, Tel: +41 26 300 8441; Email: luis.filgueira@unifr.ch
Abstract
The pectoralis major is a muscle of the upper limb girdle. This muscle has a unique morphological architectonic and a high rate of clinical applications. However, there is lack of data regarding the morphological and functional interactions of the pectoralis major with other muscle and fascial compartments. According to the applied knowledge, the “Humero-pectoral” morpho-functional concept has been postulated. The purpose of this review was the dissectible investigation of the muscle anatomy and literature review of surgical applications.
Citation
Larionov A, Yotovski P and Filgueira L. A Detailed Review on the Clinical Anatomy of the Pectoralis Major Muscle. SM J Clin Anat. 2018; 2(3): 1015.
General Anatomy
The pectoralis major is a large, flat muscle of the pectoral girdle of the upper limb. It has a fan shaped appearance with three heads or portions: the clavicular, the sternocostal and the abdominal head.
The clavicular head originates from the medial two-thirds of the clavicle (collar bone). The muscle fibers of the clavicular head have a broad origin on the caudal-anterior and caudal-posterior surface of the clavicle covering approximately half to two-thirds of that surface and converting toward the humerus, resulting in a triangular shape [1]. The clavicular head is an independent portion of the pectoralis major (Figure 1).

Figure 1: Overview of the anatomy of the pectoralis major on cadaveric prosections. (A) Anterior view of the three portions of the pectoralis major: the clavicular (CL) head, the sternocostal (SC) head and abdominal (AB) head. (B-C) Posterior view of the separated and laterally dislocated clavicular head (posterior view) with its independent, superficial, rather muscular tendon (green arrow, approx. 2.5-3.0 cm) that fuses with the tendon of the other portions shortly before the insertion; (D) Posterior view: The abdominal part has got two overlaping layers of the muscle fibres; (E) The three heads have a joint insertion of approximately 3.0-5.0 cm onto the crest of the greater tubercle of the humerus (purple double arrow). Other structures: deltoid muscle (DM), biceps brachii muscle (BBM), clacicle (C), head of humerus (HH), pectoralis minor muscle (PmM).
It is located more superficial and partially overlapping ventrally the sternocostal head. According to our observations, the clavicular portion has an autonomous tendon of approximately 3.0cm length. This distinct tendon enters in contact towards the insertion on the humerus with the tendon of the sternocostal and abdominal parts.
The sternocostal head originates from the manubrium and the body of sternum, as well as from the cartilages of the first six ribs. This part is the largest, thickest and strongest portion of the pectoralis, usually well developed in athletes [2]. Detailed dissection revealed that the sternocostal portion includes about three muscular clusters with well-pronounced interstitial clefts (Figure 1C).
The third element of the pectoralis major is the abdominal head. This part originates from the tendinous sheath of the rectus abdomen is [3] and/or superficial aponeurosis of external oblique [4]. The abdominal head has two layers of muscle fibers, which wind around each other towards its tendon, as well as around the caudal edge of sternocostal head (Figure1D).
Tendon Anatomy
The tendon of the pectoralis major has a “convoluted” appearance. According to the literature it consists of two layers [5,6]. The clavicular tendon constitutes the first layer. The second layer is the common tendon from the sternocostal and abdominal portions. The layers screw around each other and as a result the common sterno-costo-abdominal portion fixes more distally to the humerus compare to the clavicular portion which fixes a bit proximally [7,8]. In literature, the different layers are named as anterior and posterior layers (lamina). In cadaver dissection, we correspondingly observed complex organization of the pectoralis major tendon. The three muscular portions together forma broad, flat, strong tendon that extends along the crest of the major tubercle of the humerus, close to the bicipital groove (intertubercular sulcus), which varies in size between 3.0-5.0 cm (Figure 1E). However, the tendinous fibres of the three portions form three distinct layers that can be easily separated anatomically. The tendinous fibres of the three layers have different orientations in continuity of and according to the different orientation of the muscle fibres of the three heads, i.e. cranial-medial to caudal-lateral for the clavicular head, horizontal for the sternocostal head, caudal-medial to cranial-lateral for the abdominal head. This allows pulling on the proximal humerus in three different direction, i.e. proximal direction for the clavicular head, plain adduction for the sternocostal head and distal direction for the abdominal head. Together, they allow better stabilisation of the upper arm in the adduction position. The specific tendon architecture of the pectoralis major allows surgeons to use different portions as independent muscles for shoulder joint or reconstructive surgery. In the literature, there are some descriptions of pectoralis major communication with other muscles and tendons. A unique variant of an accessory tendon portion that extends from the lateral part of the pectoralis major to the capsule of the shoulder joint was described by Hammed and Mohammed [1]. The accessory tendon was connected to the long head of the biceps brachii. We observed the tendon of the abdominal portion to communicate with the synovial vagina of the long head of the biceps brachii (Figure 2A).

Figure 2: Anterior view of the fascio-tendoneousbridge (arrow) between the deltoidmuscle (DM) tendon and the tendon of the clavicular head of pectoralis major (PM).Other structures: Sternocostal head of pectoralis major muscle (SC), biceps brachii muscle (BBM), tendon of short head of biceps brachii muscle (TsBB), pectoralis minor muscle (PmM).
Other dissection revealed insertion of the common pectoral tendon onto the lateral lip (crest) of the intertubercular sulcus (bicipital groove) (Figure 2B). The thick and large common tendon from three portions communicated with the deltoid tendon (Figure 3).

Figure 3: Anterior view of the proximal left upper arm and posterior view of the pectoralis major musle (laterally folded). (A) The tendon of the abdominal head (AB) connects to the synovial vagina (arrow) of the long head of the biceps brachii (LhBB). (B) Pectoral tendon fixes to the lateral lip of the intertubercular sulcus (bicipital groove, arrow). Other structures: Sternocostal head of the pectoralis major muscle (ST), clavicle (C), latissimus dorsi muscle (LD), coracobrachial muscle (CBM), deltoid muscle (DM).
Moreover, the proximal third of the common pectoralis tendon can be connected to the coracobrachialis and the short head of bicepsbrachii. In that case, the tendon extents to the coracoid process, the origin of the two muscles (Figure 4).

Figure 4: Medial view of the proximal left upper arm. The tendon of the abdominal head of the pectoralis major interacts with the coracobrachialis (CB) and the short head of biceps brachii (ShBB). Then it continues onto the coracoid process (CP, arrow). Other structures: Sternocostal head of the pectoralis major muscle (ST), pectoralis minor muscle (PmM), clavicle (C).
Fascial Anatomy
From literature, it is known that the pectoralis major is covered by a thin enveloping pectoral fascia (also called thoracic fascia), which originates from the clavicle and sternum and is in continuity with the facial layer that covers the muscles of the shoulder, thorax, abdomen, and back [9,10]. We observed that the pectoral fascia is a dissimilar element, which creates an individual fascial bed for the clavicular, sternocostal and abdominal portions. These fascial beds are separated from each other by connective septa; they can be easily torn apart by the blunt part of the scalpel. This connective tissue space allows the three portions to move separately and to glide against each other (Figure 1).
At the caudal border of the pectoralis major, the fascia divides into a superficial and a deeper layer: the superficial fascia covers the superficial part of the pectoralis major, the deeper layer rolls back the muscle and intercommunicates with the fascia of the pectoralis minor and the coracoclavicular fascia (clavipectoral fascia) [10]. The thickness of the thoracic fascia is not constant; it varies from 0.2 to 0.5 mm in different sites of the fascia (caudal, medial and lateral). The pectoral part of thoracic fascia fibers direction is perpendicular to the direction of pectoralis major muscle fibers [9]. Histologically, the superficial fascia of the pectoralis major is a connective tissue, which contains abundant elastic fibers linked with collagen fibers. The deeper fascia of pectoralis major is anepimysial fascia type with a collagenous layer of approximately 150-200 μm thickness [11]. According to other publications of A. Stecco, the fascial tissue should be regarded not only as a primitive muscle stabilizing element of the locomotion system, but also as a “dynamic tissue” which participates in the blood supply and innervation of underlying muscles [12].
In routine dissections, we observed that muscles of the pectoral girdle, especially the pectoralis major, interact with each other through the fascial fibers. Thus, we found the fascial interaction between the pectoralis major and supraspinatus, as well as the infraspinatus, the teres minor and the deltoid (Figure 2). The deltoid sends fascial and tendinous bridges to the pectoralis major tendon (pic 3A-B). Moreover, the humeral capsule can communicate with other muscles of pectoral girdle through the fascial fibers
Based on the demonstrated data, we postulate the “humero pectoral” morpho-functional concept of myofascial interaction. That has an applied significance in the explanation of pain syndrome in intact muscles, which have connections with the injured pectoralis major, or other muscles of the pectoral girdle. This approach is realized in the musculoskeletal rehabilitation and therapy of the damaged area. It provides new perspectives for orthopedic surgery.
Muscular Ensembles of the Upper Limb Girdle
The pectoralis major has got strong relationships with other muscles of the shoulder and upper arm: the deltoid, the biceps brachii and the latissimus dorsi [4]. These muscles work together, either in an agonistic or in an antagonistic way.
One of the first attempts to distinguish anatomical interrelations has been published in 19 century by J. B. Perrin from the King’s College of London. The author pointed out that the interaction between the upper limb and the pectoral muscles is characterized by the anatomical communications between the pectoralis major and the deltoid (deltopectoral), as well as between the pectoralis major and the biceps brachii (brachiopectoral).
For the deltopectoral relationship, different variations have been described: (1) the pectoral muscle (a part or the whole muscle) blends with the deltoid at the humeral attachment; (2) the clavicular portion of the pectoral muscle merge entirely with the deltoid, which then separates from the sternocostal portion by an inconstantly sized cleft; (3) The pectoralis major and deltoid muscle are completely merged and there is no cleft between the two muscles [13].
The brachiopectoral relationship is characterized by the following variants. Firstly, the pectoralis major insets onto the “bicipital bridge”. In this type of intermuscular communication, the clavicular part consists of an external and an internal slip, whereby the external slip goes dorsal to the long head of the biceps and the internal slip keeps the classic fixation pattern [13]
The multifaceted relationships of the pectoralis major with other muscles and the gleno-humeral joint through the fascial skeleton was detected in several dissections (not shown). We observed the indivisible complex of the “fascial-muscular-tendon-ligament” apparatus, which provides the vital functions of the humeral joint
Another case revealed that the long head of the biceps brachii originates from the supraglenoid tubercle and gave fibers of connective tissue to the capsule of the humeral joint. The short head starts from the coracoid process and send the fibers to the capsule of humeral joint (not shown).
Development
Most of the variations of the pectoralis major could be understood through looking into its development. Unfortunately, there is not much known in human and more studies are needed. However, from the perspective of comparative anatomy and for better understanding of the development, the muscles of the shoulder and the pectoral region can be classified as scapulohumeral, axiohumeral and axioscapular conglomerates. The scapulohumeral group consists of the muscles, which connect the humerus to the scapula, including the supraspinatus, infraspinatus, teres minor, teres major, subscapularis and deltoid. The axioscapular group is responsible for the primary shoulder function, and consists of serratus anterior, rhomboideus, levator scapulae and trapezius. Muscles of the axiohumeral group extend from the trunk to the humerus [14], including the pectoralis major and the latissimus dorsi. As all striated skeletal muscle, the pectoralis major developed from the paraxial mesoderm [15]. So, already at week5 of embryologic development, the pectoral pre muscle mass derives from the second thoracic segment. The median part is attached to the clavicle and later develops into the clavicular and sternocostal portion [8]. According to the comparative anatomy concept, a precursor of pectoral muscles is a “primitive muscle layer” linking the coracoid with the humerus. Evolutionary, in the later reptilian and early mammalian animals, the part from ”primitive muscle” displaces into the dorsal direction and attaches to the scapula (this portion gives development to supraspinatus, infraspinatus subscapularis) meanwhile another part of “primitive layer” migrates from the procoracoid to the sternum and becomes the pectoralis major. Interestingly, published and our dissection findings (variations of pectoralis major interacting with the scapula-humeral muscles) are in concordance with the comparative anatomy concept [14]
Innervation and Blood Supply
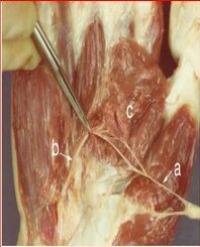
The blood supply and innervation of the pectoralis major have important significance for surgery. However, the supply of the nerves and vessels to the muscles is pronouncedly individual. The standard anatomical innervation of the pectoralis major is provided by the medial and the lateral pectoral nerves [3,4]. The lateral pectoral nerve arises in 88% from the lateral cord of the brachial plexus and in 12 % from the medial cord of the brachial plexus. It provides the innervation for the clavicular portion [16,17]. In 76 %, the medial pectoral nerve provides first the main branch to the pectoralis minor muscle, before it continues and subdivides into the abdominal and sternal portions of the pectoralis major. In 34 %, the medial pectoral nerve splits into several branches before entering in the musculus pectoralis minor [16-19]. The medial pectoral nerve is located medially to the axillary artery and in 88 % takes its origin from the medial cord of the brachial plexus. Visually, the medial pectoral nerve is thinner than the lateral pectoral nerve [20,21]. The medial pectoral nerve mostly innervates caudal segments of the muscle: i.e. the sternocostal and abdominal portions [17,21].
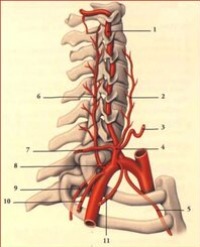
Mostly, four arteries participate in the blood supply of the pectoralis major, including the thoracoacromial artery, the lateral and superior thoracic artery, as well as the intercostal arteries [3,22]. The thoracoacromial artery is a branch of the axillary artery, of which the thoracoacrominal pedicule is usually located within the space enclosed by the clavicle, the acromioxy phoid line and medclavicular line [23]. However, in some cases, the thoracoacromial peduncle is located laterally to the acromioxyphoid line that should be taken into consideration by the surgeons [24]. In most cases, the lateral thoracic artery goes with the medial pectoral nerve and should be regarded as a factor of a potential risk of injury during surgical separation of the portions of the pectoralis major [16].
Function
As mention before, the pectoralis major is a complex muscle, which consists of three independent portions. Functionally these portions play an independent role and participate in diverse movements
The clavicular portion together with clavicular part of the deltoid participates in adduction and elevation of the arm. It brings the upper arm back from external rotation to the neutral position. This portion is involved in low range of motions with the elevation of the arm, e.g., touching the chin etc [25].
The sternoclavicular portion provides mostly adduction with internal rotation.
The abdominal portion contributes to depression of the arm and it supports push-up movements in the neutral position.
In the neutral position, the main antagonists for the pectoralis major are the deltoid (acromial and spinal parts) and the supraspinatus. The agonists are the subscapularis, the teres minor and major, as well as partially the latissimus dorsi [26] (Table 1).
Table 1: Functional agonists and antagonists of the pectoralis major adapted from Vankov and Ovcharov2008, Sinelnikov 1988
|
|
Abduction
|
Adduction
|
Internal rotation
(pronation)
|
External
rotation (supination)
|
Anteflexio (flexion)
|
Retroflexio
(extension)
|
Forward or
Backward elevation
|
Forward or Backward
depression
|
|
Pectoralis major
(whole muscle)
|
|
+
|
+
|
|
|
|
|
|
|
Pectoralis major
(clavicular part)
|
|
|
|
|
|
|
+
(Forward)
|
|
|
Pectoralis major
(sternocostal part)
|
|
+
|
|
|
|
|
|
|
|
Pectoralis major
(abdominal part)
|
|
+
|
|
|
|
|
|
+
(Forward)
|
|
Deltoid
(whole muscle)
|
+
|
+
(NB: in case of elevation the arm till 60°)
|
|
|
|
|
|
|
|
Deltoid
(clavicular part)
|
|
|
+
|
|
+
|
|
|
|
|
Deltoid (acromial part)
|
+
(in case of elevation till 90°)
|
|
|
|
|
|
|
|
|
Deltoid
(spinal part)
|
|
|
|
+
|
|
+
|
|
|
|
Supraspinatus
|
+
|
|
|
+
|
|
|
|
|
|
Infraspinatus
|
|
|
|
+
|
|
|
|
|
|
Teres minor
|
|
+
|
|
+
|
|
|
|
|
|
Teres major
|
|
+
|
+
|
|
|
+
|
|
|
|
Subscapularis
|
|
+
|
+
|
|
|
|
|
|
|
Latissimus dorsi
|
|
+
|
+
|
|
|
|
+
(Forward and Backward)
|
+
(Forward and Backward)
|
In general, the pectoralis major is a robust adductor, which participates in the internal rotation and flexion in the glenohumeral joint. This muscle is significant for the “dynamic stabilization” of the arm and shoulder; it plays an important role from a structural point of view in the anterior axillar wall formation and from a functional point of view in the specific pitching actions [27], the pull-up and push-up exercises, climbing or even respiration with fixed arms. This muscle is an important driving element for tennis players, athletes-throwers (discus, javelin, hammer, etc.), dart players, baseball and basketball players, golf-players, sprinters, etc. The “throwing movements” as a principal function of the shoulder girdle requires all three portions of the pectoralis major. The kinetic chain of the “throwing motion” contains four consistent movements: (1) the wind up (a shoulder abduction, extension, external rotation together with lateral trunk f lexion), the cocking (a maximal external rotation and the increased scapular rotation), the acceleration (internal rotation and adduction of the shoulder) and the follow-through (the maximal internal rotation of the shoulder, adduction of the shoulder and decreased activity of the muscles) [28,29]. The pectoralis major together with the latissimus dorsi and the subscapularis takes part in the acceleration stage of the throwing. Minimal activation of the pectoralis major was registered at the wind-up and the cocking stages [30].
Lack or Loss of Function
The functional insufficiency of the pectoralis major is usually a result of sport trauma or congenital malformation affecting the muscle itself, or deficiency in its blood or nerve supply
The rupture of the pectoralis major muscle is the most frequent type of the injury. The first observation of this type of dysfunction was first described by Patissier et al. in the beginning of 19 century [31]. The most defined cases have been registered among athletes, weight lifters, windsurfers, victims of violence and motor car accidents [32 35]. Rupture of the pectoralis major due to car accidents has been allocated to the seat belt [36]. The central mechanism of a complete disruption is overloading of the contracted muscle with concurrent external rotation and abduction of the arm [27,37]. The clinical injury classification is based on the degree of the muscle damage: type I (muscle strain); type II (partial tear); type III (complete tear). The total rupture is subdivided according to injury localization IIIA (muscle rapture); IIIB (muscle belly rupture); IIIC (musculotendinous junction rupture) and IIID (rupture of the tendon) [38]. The musculotendinous and bony avulsion junction are the most typical places of tears for the pectoralis major. According to the data of Bak et al. (2000), bony avulsion occurs in younger individuals before the age of 30 years and correlates with sport activity; the musculotendinous avulsion happens more often after the age of 30 years and relates to professional aspects [7]. The tendon insertion of the pectoralis major into the bone is frequent injury localization in seniors; the pectoralis major rupture of muscle belly is quite rare [39].
The patients usually are able to hear the clicking noise with the tearing sensation during the injury event [40]. The main clinical signs of the pectoralis major avulsion are variable and determined by localization and degree of injury. The most frequent clinical signs are an ecchymosis (lateral and anterior surfaces), sudden and aching pain localized high up medially in the arm, functiolaesa (inward rotation and adduction are substantially reduced), oedema and weakness. During the examination palpable defect of the muscle and asymmetry in the shape of the chest wall can be detected [41-44].
Complications of the pectoralis major ruptures are rare and can be divided into routine and deferred. The most well known routine complication is an action dysfunction. However, some of the patients keep the normal function after the muscle tear [45]. The typically deferred complication is the calcification of the injury side if not treated surgically, as well as the loss of its primary function [46], suppuration [47] or even development of rhabdomyosarcoma [48,49].
A functional abnormality can also be caused by the congenital absence of the pectoralis major. The congenital lack of the pectoralis major is often associated with hand anomalies such as the Polland’s syndrome [50,51] renal anomalies [52], or Klippel-Feil anomaly [53]. Some patients with pectoral major aplasia (hypoplasia) demonstrate the inability to rotate the shoulder and upper arm internally (Poland's syndrome Ireland) and the deficiency of horizontal adduction movement; the adduction strength is lost up to 20 %- 30 % [54]. T he absence of the different portions of the pectoralis major can be substituted by other muscles: clavicular deltoid replaces clavicular portion [5], latissimus dorsi can substitute functional in sufficiency of the abdominal and sternocostal portions [55]. However, in most cases, patients with congenital absence of the pectoralis major do not present any functional deficiency of the upper limb for daily movements, but demonstrate a strongly visible esthetic defect of the breast [56].
Treatment and Rehabilitation after Injury
The pectoralis major tear is a rare and irregular injury. The muscle is an integral part of the occasional personal activity; it plays a vital role in strenuous work or sport. The surgical treatment of the functional deficiency is preferred in patients with complete rupture and not essential for the partly disrupted muscle which mostly is submitted to nonoperative treatment.
The nonsurgical treatment consists of the following steps: immobilization for 2-4 weeks, application of cryotherapy, control of the hematoma and analgesia prescription.
The invasive intervention is standardized for the treatment of professional sportsmen. According to the data of M. Jones et al. [40], the results of medical intervention correlate with time passed after the accident. So, surgical treatment within the first week after injury is more effective and results in full recovery of the movement and power without development of a pain syndrome. Surgery performed two weeks after injury is characterized by the full return of motion with development of a mild pain syndrome. Surgery eight-months after injury results in reduced motional activity with the development of a troublesome pain syndrome and weakness of the upper arm. Surgical treatment pursues to eliminate the cosmetic breast deformation and to accelerate the functional recovery of the upper limb. The typical surgery manipulation adds up to the mobilization and fixation of the identified disrupted tendon part. The deltopectoral surgical access is a typical place of the incision [57]. To avoid the early failure, it is necessary to control the efficiency of the tendon reparation and estimate the function of the extremity after repair, but before the wound closure. For these purpose, the surgeon can perform 30° shoulder external rotation [58].
The rehabilitation approach after surgery or for conservative therapy is similar. In both cases, the aim is limb function improvement, maximal non-painful mobility and the recovery of the damaged muscle power.
The rehabilitation period includes: (1) immediate post-operative step (0-2 weeks), intermediate post-operative step ( 3-7 weeks), (2) late post-operative step (7-12 weeks) and (3) advanced strengthening step (12 and more weeks) [59-61]. The first two weeks, the patients are immobilized with a sling. This time is important for the identification of the range of possible active motions. The following 3-7 weeks are characterized the by the application of the moderate resistance exercise with the initial adduction and internal rotation. At 7-12 weeks the activities for a full range of motion are performed. The advanced step (after 12 weeks) includes the complex of the movement for developing of the flexibility, power, and endurance [58,59,62,63].
Rehabilitation of the congenital pectoralis major abnormalities aims mostly for the elimination of the cosmetic defects. The inherited malformations, as mentioned before, do not provoke any severe functional lacks; the light motional dysfunction is very well compensated by other muscles in this case [64]. For the elimination of the esthetic deficiency, the transfer of the latissimus dorsi to the pectoralis major can be used [55]. However, the functional aspect of the latissimus dorsi application is discutable. The latissimus dorsi is responsible for elevation and depression of the upper extremity and utilization of this muscle for aesthetic surgery can provoke the weakness of dorsal extension and depression from anterior elevation, as well as internal rotation.
Using the Pectoralis Major as Graft and for Replacement Therapy
The anatomy of the pectoralis major has a unique organization and function that can be partially compensated by other muscles, as mentioned above. Three different portions, unique blood supply, and innervation allow this muscle to be used as local autologous “spare” tissue in orthopedic and reconstructive surgery. Consequently, the pectoralis major has been successfully used for the replacement of other more important muscles with functional dysfunction of different etiology, as well as palsy or ruptures. The pectoralis major is an option for the repair of various organic defects caused by trauma or iatrogeny [65]. The first data about the surgical substitution of the muscle were published in the 30s of the XX century. Durman et al. (1945) described the use of the pectoralis major for replacement of the paralyzed serratus anterior [66]. This muscle has been used for scapular winging stabilization [67]. The entire pectoralis major has also been used for the replacement and reconstruction of the biceps brachii [68]. The sternoclavicular portion of the pectoralis major has been used for the elimination of the anterolateral deltoid deficiency [69], the sternocostal and clavicular portions have been used for the treatment of irreversible rupture of the subscapularis tendon [16,60,70-74]. Moreover, the different portions of the pectoralis major have been used in head and neck, chest wall and upper limb orthopedic surgery [2,75-78]. Deficiency of the rotator cuff of the shoulder has been treated with the combined transfer of the latissimus dorsi and the pectoralis major [79].
Conclusion
The pectoralis major is a multifunctional acting muscle. It provides not only functional support of upper limb and shoulder, but plays an important role in aesthetic appearance. Clinical anatomy knowledge about the pectoralis major is essential for the appreciation of the functional and structural characteristics of the upper limb region.
The pectoralis major is a vital functional muscle for athletes, tennis players, golf players and specific for certain professional activities (e.g., agriculture, lifting a baby). The muscle is a unique element of the humero-pectoral system providing not only direct adduction, internal rotation, and flexion (elevation) in the glenohumeral joint, but it supports dynamic stability, appropriate arthrokinetics and plays the role of a humeral flexibility propagator. Three independent muscle portions of the pectoralis major are an indispensable source for transplantation in specific injuries or functional dysfunctions and cosmetic deformity.
Acknowledgements
We thank Marco Gagliano and Franz Jungo for their excellent technical support. The work has been funded by the University of Fribourg.
References
1. Hammad RB, Mohamed A. Unilateral four-headed pectoralis muscle major. Mcgill J Med. 2006; 9: 28-30.
2. Withers EH, Franklin JD, Madden JJ, Lynch JB. Pectoralis major musculocutaneous flap: A new flap in head and neck reconstruction. Am J Surg. 1979; 138: 537-543.
3. Sinelnikov RD. Atlas of human anatomy. 5th edn. Moscow: Mir Publishers. 1988; 453.
4. Standring S. Gray’s Anatomy: The Anatomical Basis of Clinical Practice. 40th edn. Borley N, Patricia C, Alan C, Michel G, editors. Churchill Livingstone Elsevier. 2009; 2671.
5. Barberini F. The clavicular part of the pectoralis major: a true entity of the upper limb on anatomical, phylogenetic, ontogenetic, functional and clinical bases. Case report and review of the literature. Ital J Anat Embryol. 2014; 119: 49-59.
6. Aärimaa V, Rantanen J, Heikkilä J, Helttula I, Orava S. Rupture of the pectoralis major muscle. Am J Sports Med. 2004; 32: 1256-1262.
7. Bak K, Cameron EA, Henderson IJ. Rupture of the pectoralis major: a meta analysis of 112 cases. Knee Surg Sports Traumatol Arthrosc. 2000; 8: 113 119.
8. Paraskevas GK, Raikos A. Bilateral pectoral musculature malformations with concomitant vascular anomaly. Folia Morphol (Warsz). 2010; 69: 187-191.
9. Jinde L, Jianliang S, Xiaoping C, Xiaoyan T, Jiaqing L, Qun M, et al. Anatomy and Clinical Significance of Pectoral Fascia. Plast Reconstr Surg. 2006; 118: 1557-1560.
10. Gray H, Lewis WH. Anatomy of the human body. 20th. Lewis BH, editor. Philadelphia and New York: Lea & Febiger; 1918. 1396.
11. Stecco A, Macchi V, Masiero S, Porzionato A, Tiengo C, Stecco C, et al. Pectoral and femoral fasciae: common aspects and regional specializations. Surg Radiol Anat. 2009; 31: 35-42.
12. Stecco C, Stern R, Porzionato A, Macchi V, Masiero S, Stecco A, et al. Hyaluronan within fascia in the etiology of myofascial pain. Surg Radiol Anat. 2011; 33: 891-896.
13. Perrin JB. Notes on some Variations of the Pectoralis Major, with its Associate Muscles. J Anat Physiol. 1871; 5: 233-420.
14. DePalma AF. The classic. Origin and comparative anatomy of the pectoral limb. Surgery of the shoulder. Clin Orthop Relat Res. 2008; 466: 531-542.
15. Sadler TW. Langman’s medicla embrology. Taylor C, editor. 12th edn. Wolters Kluwer Lippincott Williams & Wilkins. 2012; 384.
16. Nelson GN, Namdari S, Galatz L, Keener JD. Pectoralis major tendon transfer for irreparable subscapularis tears. J shoulder Elb Surg. 2014; 23: 909-918
17. Prakash KG, Saniya K. Anatomical study of pectoral nerves and its implications in surgery. J Clin Diagn Res. 2014; 8: 1-5.
18. Klepps SJ, Goldfarb C, Flatow E, Galatz LM, Yamaguchi K. Anatomic evaluation of the subcoracoid pectoralis major transfer in human cadavers. J shoulder Elb Surg. 2001; 10: 453-459.
19. Resch H, Povacz P, Maurer H, Koller H, Tauber M. Pectoralis major inverse plasty for functional reconstruction in patients with anterolateral deltoid deficiency. J Bone Joint Surg Br. 2008; 90: 757-763.
20. Corten E, Schellekens P, Bleys R, Kon M. The nerve supply to the clavicular part of the pectoralis major muscle: an anatomical study and clinical application of the function-preserving pectoralis major island flap. Plast Reconstr Surg. 2003; 112: 969-975.
21. Scevola S, Cowan J, Harrison DH. Does the removal of pectoralis minor impair the function of pectoralis major? Plast Reconstr Surg. 2003; 112: 1266-1273.
22. Manktelow RT, McKee NH, Vettese T. An anatomical study of the pectoralis major muscle as related to functioning free muscle transplantation. Plast Reconstr Surg. 1980; 65: 610-615.
23. Benhamed L, Bellier J, Hysi I, Lopez B, Wurtz A. Harvest technique for pedicled intrathoracic transposition of pectoralis major muscle. Gen Thorac Cardiovasc Surg. 2012; 60: 546-548.
24. Ben Hadj Yahia S, Vacher C, Guédon C. Étude anatomique de la localisation du pédicule thoracoacromial. Intérêt dans les lambeaux musculocutanés de grand pectoral. Morphologie. 2009; 93:13-19.
25. Gowland C, DeBruin H, Basmajian J V, Plews N, Burcea I. Agonist and antagonist activity during voluntary upper-limb movement in patients with stroke. Phys Ther. 1992; 72: 624-633.
26. Vankov V, Ovcharov V. Human anatomy (in bulgarian: Анатомияначовека). 10th edn. Sophia: Arso, Sopiya; 2008. 936.
27. Quinlan JF, Molloy M, Hurson BJ. Pectoralis major tendon ruptures: when to operate. Br J Sports Med. 2002; 36: 226-228.
28. Wilk KE, Meister K, Fleisig G, Andrews JR. Biomechanics of the Overhead Throwing Motion. Sports Med Arthrosc. 2000; 8: 124-134.
29. Erickson BJ, Thorsness RJ, Hamamoto JT, Verma NN. The biomechanics of throwing. Sports Med Arthrosc. 2016; 24: 156-161.
30. Ryu RK, McCormick J, Jobe FW, Moynes DR, Antonelli DJ. An electromyographic analysis of shoulder functions in tennis players. Am J Sports Med. 1988; 16: 481-485.
31. Pochini A, Ejnisman B, Andreoli CV, Monteiro GC, Silva AC, Cohen M, et al. Pectoralis major muscle rupture in athletes: a prospective study. Am J Sports Med. 2010; 38: 92-98.
32. Kawashima M, Sato M, Torisu T, Himeno R, Iwabuchi A. Rupture of the pectoralis major. Report of 2 cases. Clin Orthop Relat Res. 1975; 28: 115 119.
33. Pochini AC, Ejnisman B, Andreoli CV, Monteiro GC, Fleury AM, Falappa F et al. Exact moment of tendon of pectoralis major muscle rupture captured on video. Br J Sports Med. 2007; 41: 618-619.
34. Kircher J, Ziskoven C, Patzer T, Zaps D, Bittersohl B, Krauspe R. Surgical and nonsurgical treatment of total rupture of the pectoralis major muscle in athletes: update and critical appraisal. Open access J Sport Med. 2010; 1: 201-205.
35. Dunkelman NR, Collier F, Rook JL, Nagler W, Brennan MJ. Pectoralis major muscle ruptures in windsurfing. Arch Phys Med Rehabil. 1994; 75: 819-821.
36. Harvey KP, Adair JD, Ali MA. Seat belt trauma: pectoralis muscle rupture and delayed mesh repair. J Trauma. 2008; 64: 831-833.
37. Pavlik A, Csépai D, Berkes I. Surgical treatment of pectoralis major ruptures in athletes. Knee Surg Sports Traumatol Arthrosc. 1998; 6: 129-133.
38. Merolla G, Paladini P, Campi F, Porcellini G. Pectoralis major tendon rupture. Surgical procedures review. Muscles Ligaments Tendons J. 2012; 2: 96-103.
39. Goriganti MR, Bodack MP, Nagler W. Pectoralis major rupture during gait training: case report. Arch Phys Med Rehabil. 1999; 80: 115-117.
40. Jones MW, Matthews JP. Rupture of pectoralis major in weight lifters: a case report and review of the literature. Injury. 1988; 19: 219.
41. Bakalim G. Rupture of the pectoralis major muscle. A case report. Acta Orthop Scand. 1965; 36: 274-279.
42. Ryan SA, Bernard AW. Pectoralis major rupture. J Emerg Med. 2011; 40: 208-209.
43. Tietjen R. Closed injuries of the pectoralis major muscle. J Trauma. 1980; 20: 262-264.
44. Berson BL. Surgical repair of pectoralis major rupture in an athlete. Am J Sports Med. 1979; 7: 348-351.
45. Pochini AC, Rodrigues MBR, Yamashita L, Belangero PS, Andreoli CV, Ejnisman B. Surgical treatment of pectoralis major muscle rupture with adjustable cortical button. Rev Bras Ortop. 2018; 53: 60-66.
46. Purnell R. Rupture of the pectoralis major muscle: a complication. Injury. 1988; 19: 284.
47. Pai VS, Simison AJ. A rare complication of pectoralis major rupture. Aust N Z J Surg. 1995; 65: 694-5.
48. Smith FC. Rupture of the pectoralis major muscle: a caveat. Injury. 1988; 19: 282-283.
49. Van Mater D, Añó L, Blum JM, Webster MT, Huang W, Williams N et al. Acute tissue injury activates satellite cells and promotes sarcoma formation via the HGF/c-MET signaling pathway. Cancer Res. 2015; 75: 605-614.
50. David TJ, Winter RM. Familial absence of the pectoralis major, serratus anterior, and latissimus dorsi muscles. J Med Genet. 1985; 22: 390-392.
51. Mace JW, Kaplan J, Schanberger JE, Gotlin RW. Poland’s Syndrome. Report of Seven Cases and Review of the Literature. Clin Pediatr (Phila). 1972; 11: 98-102.
52. Hegde HR, Leung AK. Aplasia of pectoralis major muscle and renal anomalies. Am J Med Genet. 1989; 32: 109-111.
53. Hegde HR, Shokeir MH. Posterior shoulder girdle abnormalities with absence of pectoralis major muscle. Am J Med Genet. 1982; 13: 285-293.
54. Mysnyk MC, Johnson DE. Congenital absence of the pectoralis muscles in two collegiate wrestling champions. Clin Orthop Relat Res. 1991; 265: 183-186.
55. Ohmori K, Takada H. Correction of Poland’s pectoralis major muscle anomaly with latissimus dorsi musculocutaneous flaps. Plast Reconstr Surg. 1980; 65: 400-404.
56. Karnak I, Tanyel FC, Tunçbilek E, Ünsal M, Büyükpamukçu N. Bilateral Poland anomaly. Am J Med Genet. 1998; 75: 505-507.
57. Griffiths GP, Selesnick FH. Rupture of the Pectoralis Major Muscle. Phys Sports med. 1997; 25: 118-125.
58. Vasiliadis AV, Lampridis V, Georgiannos D, Bisbinas IG. Rehabilitation exercise program after surgical treatment of pectoralis major rupture. A case report. Phys Ther Sport. 2016; 20: 32-39.
59. Manske RC, Prohaska D. Pectoralis major tendon repair post surgical rehabilitation. N Am J Sports Phys Ther. 2007; 2: 22-33.
60. Shin JJ, Saccomanno MF, Cole BJ, Romeo AA, Nicholson GP, Verma NN. Pectoralis major transfer for treatment of irreparable subscapularis tear: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2016; 24: 1951 1960.
61. Galatz LM, Connor PM, Calfee RP, Hsu JC, Yamaguchi K. Pectoralis major transfer for anterior-superior subluxation in massive rotator cuff insufficiency. J Shoulder Elb Surg. 2003; 12: 1-5
62. Hoppes CW, Ross MD, Moore JH. Undetected pectoralis major tendon rupture in a patient referred to a physical therapist in a combat environment: a case report. Phys Ther. 2013; 93: 1225-1233.
63. Butcher JD, Siekanowicz A, Pettrone F. Pectoralis major rupture: ensuring accurate diagnosis and effective rehabilitation. Phys Sports med. 1996; 24: 37-44.
64. Engber WD. Cleft hand and pectoral aplasia. J Hand Surg Am. 1981; 6: 574 577.
65. Siu K-F, Wei WI, Lam K-H, Wong J. Use of the pectoralis major muscle flap for repair of a tracheoesophageal fistula. Am J Surg. 1985; 150: 617-619.
66. Durman DC, Michigan S. An operation for paralysis of the serratus anterior. J bone Jt Surg. 1945; 27: 380-382.
67. Tauber M, Moursy M, Koller H, Schwartz M, Resch H. Direct pectoralis major muscle transfer for dynamic stabilization of scapular winging. J Shoulder Elb Surg. 2008; 17: 29-34.
68. Carroll RE, Kleinman WB. Pectoralis major transplantation to restore elbow f lexion to the paralytic limb. J Hand Surg Am. 1979; 4: 501-507.
69. Resch H, Povacz P, Maurer H, Koller H, Tauber M. Pectoralis major inverse plasty for functional reconstruction in patients with anterolateral deltoid deficiency. J Bone Joint Surg Br. 2008; 90: 757-763.
70. Jennings GJ, Keereweer S, Buijze GA, De Beer J, DuToit D. Transfer of segmentally split pectoralis major for the treatment of irreparable rupture of the subscapularis tendon. J shoulder Elb Surg. 2007; 16: 837-842.
71. Elhassan B, Ozbaydar M, Massimini D, Diller D, Higgins L, Warner JJP. Transfer of pectoralis major for the treatment of irreparable tears of subscapularis: does it work? J Bone Joint Surg Br. 2008; 90: 1059-1065.
72. Konrad GG, Sudkamp NP, Kreuz PC, Jolly JT, McMahon PJ, Debski RE. Pectoralis major tendon transfers above or underneath the conjoint tendon in subscapularis-deficient shoulders. An in vitro biomechanical analysis. J Bone Jt Surg. 2007; 89: 2477-2484.
73. Valenti P, Boughebri O, Moraiti C, Dib C, Maqdes A, Amouyel T, et al. Transfer of the clavicular or sternocostal portion of the pectoralis major muscle for irreparable tears of the subscapularis. Technique and clinical results. Int Orthop. 2015; 39: 477-483.
74. Jost B, Puskas GJ, Lustenberger A, Gerber C. Outcome of pectoralis major transfer for the treatment of irreparable subscapularis tears. J Bone Jt Surgery-American Vol. 2003; 85: 1944-1951.
75. Tobin GR. Pectoralis major segmental anatomy and segmentally split pectoralis major flaps. Plast Reconstr Surg. 1985; 75: 814-824.
76. Kruse AL, Luebbers HT, Grätz KW, Bredell M. A new method for closure of large donor side defects after raising the pectoralis major flap. Oral Maxillofac Surg. 2011; 15: 251-252.
77. Nahai F, Morales L, Bone DK, Bostwick J. Pectoralis major muscle turnover f laps for closure of the infected sternotomy wound with preservation of form and function. Plast Reconstr Surg. 1982; 70: 471-474.
78. Harris PA, Kelly M, Calvert PT, Gateley D. The use of a pectoralis major muscle turnover flap to cover anterior shoulder defects after infected rotator cuff repair. J Shoulder Elb Surg. 2004; 13: 235-238.
79. Aldridge JM, Atkinson TS, Mallon WJ. Combined pectoralis major and latissimus dorsi tendon transfer for massive rotator cuff deficiency. J Shoulder Elb Surg. 2004; 13: 621-629