Case Report | Volume 1 - Issue 1 | Article DOI :
Download PDF
Aneesh Dave*, Rohan Dalal, Bardia Aryaie and Bahadir Cem Demirdes
Department of Anatomy and Histology, The University of Sydney, Australia
Corresponding Author:
Aneesh Dave, Department of Anatomy
and Histology, The University of Sydney,
Australia, P.O. Box 4270, Homebush,
NSW 2140, Australia,
Tel: +61431474787;
Email: aneesh.dave@sydney.edu.au
Keywords
Variation; Intestinal; Rectum; Duplication
Abstract
This report describes a long rectal duplication cyst found during routine dissection of an 82 year old male cadaver. The cyst was tubular, blind-ending and non-communicating. It emerged from the posterior rectal wall approximately 13cm superior to the anal verge and was 12cm in length. Long duplication cysts such as that described may cause complications such as perforation, bleeding and chronic pain. Hence duplication cysts should form part of the differential work up in a clinical setting.
Citation
Dave A, Dalal R, Aryaie B and Demirdes BC. A Long Rectal Duplication Cyst in an Adult Cadaver: A Rare Anatomical Variation. SM J Clin Anat. 2017; 1(1): 1002
Introduction
Duplication cysts are a congenital malformation which may develop along any part of the alimentary tract, occurring with an estimated prevalence of 1 in 4500 cases [1]. Duplication cysts involving the rectum are very rare, accounting for only 5% of all alimentary tract duplications [2]. Of these, 80% are spherically shaped, and 80% of patients present before two years of age [3]. Only a small number of case reports describe rectal duplication cysts presenting in adults. This case report describes a tubular, blind-ending rectal duplication cyst found during a routine dissection of an 82 year old male cadaver. Several theories have been developed to explain the embryological development of rectal duplication cysts; however none of these have been conclusive [4]. Rectal duplication cysts are an important clinical consideration, as they may result in obstruction, perforation and chronic pain [5] and must therefore be considered within a differential diagnosis framework
Case Report
Gross pelvic dissection of an 82-year old male cadaver of European ancestry was performed as per a recognized and widely used dissection manual [6], whereby a variant long rectal duplication cyst was noted. Incidentally, this cadaver was also noted to have an aberrant inferior mesenteric artery arising from the coeliac trunk. Otherwise, in life there were no significant medical issues, and there was no history of any surgical procedures to the area.
The opening of the cyst was found on the posterior aspect of the rectum, approximately 135mm superior to the anal verge (Figure 1).

Figure 1: Mid-sagittal section of pelvis showing rectal duplication cyst. A- Pubic Symphisis, B - Bladder, C- Rectum, D- Sacrum, E - Duplication Cyst, Arrow - Opening of duplication cyst into rectum.
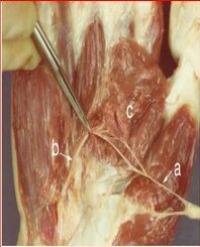
The duplication cyst was noted to be 124 mm in length,and 11.8mm in diameter. During its course, it curved around the rectosigmoid junction passing anterior to the rectum. The duplication cyst was a blind-ending, non-communicating tubular-shaped cyst. As the duplication cyst was laid open, it was noted to have a thick wall, corresponding to the multi-layered wall consistent with normal rectal lining including a mucosa and muscular layer (Figure 2).

Figure 2: Internal features of rectal duplication cyst. A- Rectum, B - Opening of rectal duplication cyst, C - Mucosal Lining of cyst
This allowed differentiation between a true duplication cyst and a simple rectal diverticulum
No other regional anatomical variants were noted. There was no significant past history of pelvic surgery or pelvic pathology associated with the cadaver.
Discussion
Duplication cysts involving the rectum are a rare congenital malformation, accounting for only 5% of all duplications in the gastrointestinal tract. Of those, the majority of cysts are reported as being within the retro-rectal space, spherically shaped, presenting in children less than two years of age and with predominance in males of European ancestry [3,7-9]. Presentation of rectal duplication in adults, as is described in this case study, has only been described within a few case reports [3,10]. The diagnosis and treatment of patients with rectal duplication cysts has advanced significantly. Most recently, endoscopic ultrasound has been used to identify rectal duplication cysts, and may provide a method of obtaining a tissue sample through fine needle aspirate [11]. Surgical excision is the treatment of choice, and this can be done through an open or endoscopic manner. Novel methods have sought to extend standard sub-mucosal endoscopic approaches to include a wide muscularis excavation [12].
The mechanism of development of rectal duplications is not fully understood, with several theories attempting to explain their formation. The mostly widely recognized theory involves an abnormality during the gastrulation stage resulting in a split notochord [4]. The herniation of the yolk sac through a gap between the ectoderm and endoderm eventually is thought to result in a yolk sac to amniotic cavity fistula, which is closed to varying degrees through continued growth of the embryo. Although this can cause duplications of the entire gastrointestinal tract, not all duplication cysts can be explained with this theory.
The presence of rectal duplication cysts should not missed, as there is a possibility of serious complications including obstruction, intussusception, infection and volvulus which may be associated with duplication cysts. The presence of ectopic gastric mucosa, which occurs in approximately a third of rectal duplication cysts [2], can also cause perforation and haemorrhage. Even if such complications are not present, constipation, chronic pain and abdominal distension can be a cause of significant morbidity to the patient [5]. In a case series of 72 patients by Stringer et al., it was noted that spinal and genitourinary anomalies were present in two of six patients, and thus further evaluation may be warranted in patients with noted rectal duplication cysts [9]. Therefore, due to the highly variable, non specific presentation, the high risk of associated co-morbidities and the difficulties in diagnostics, rectal duplication should be considered as a differential diagnosis in the refractory patient.
Acknowledgement
The authors would like to acknowledge Dinuke De Silva and Steven Gluckman for assisting with dissection.
References
1. Bond SJ, Groff DB. Pediatric Surgery. 5th edn. St Louis: Mosby. 1998.
2. Puligandla PS, Nguyen LT, St-Vil D, Flageole H, Bensoussan AL, Nguyen VH, et al. Gastrointestinal duplications. J Pediatr Surg. 2003; 38: 740-744.
3. Fotiadis C, Genetzakis M, Papandreou I, Misiakos E, Agapitos E, Zografos G. Colonic duplication in adults: report of two cases presenting with rectal bleeding. World J Gastroenterol. 2005; 11: 5072-5074.
4. Stern LE, Warner BW. Gastrointestinal Duplications. Semin Pediatr Surg. 2000; 9: 135-140.
5. Boothroyd AE, Christine MH. Rectal duplications in children: a presentation of four cases. Eur J Radiol. 1990; 10: 38-41.
6. Romanes GJ. Cunningham’s Manual of Practical Anatomy: Volume 2. Thorax and Abdomen. 15th edn. Oxford: Oxford University Press. 1986.
7. Amjadi K, Poenaru D, Soboleski D, Hurlbut D, Kamal I. Anterior rectal duplication: A diagnostic challenge. J Pediatr Surg. 2000; 35: 613-614.
8. La Quaglia MP, Feins N, Eraklis A, Hardy Hendren W. Rectal duplications. J Pediatr Surg. 1990; 25: 980-984.
9. Stringer MD, Spitz L, Abel R, Kiely E, Drake DP, Agrawal M, et al. Management of alimentary tract duplication in children. Br J Surg. 1995; 82: 74-78.
10. Reiser-Erkan C, Erkan M, Ulbrich E, Nährig J, Kleeff J. Cystic colon duplication causing intussusception in a 25-year-old man: report of a case and review of the literature. BMC Surg. 2010; 10: 1-3.
11. Castro-Pocas FM, Araujo TP, Silva JD, Goncalves VS. Endoscopic ultrasonography and rectal duplication cyst in an adult. Endosc ultrasound. 2017; 6: 336-339.
12. Ivekovic H, Bilic B, Jakic Razumovic J, Kalauz M, Rustemovic N, Piessevaux H, et al. Endoscopic muscularis excavation of a rectal duplication cyst. Endoscopy. 2015; 47: 522-524