Research Article | Volume 2 - Issue 1 | Article DOI :
Download PDF
Philippe Manyacka Ma Nyemb1,2*, Christian Fontaine3, Xavier Demondion3, Maurice Demeulaere3, Fabien Descamps3 and Jean-Marc Ndoye4
1Laboratory of Anatomy and Organogenesis, Gaston Berger University, Sénégal
2Department of General Surgery, Regional Hospital, Sénégal
3Laboratory of Anatomy, Henri Warembourg Faculty of Medicine, University of Lille 2, France
4Laboratory of Anatomy and Organogenesis, Cheikh Anta Diop University, Sénégal
Corresponding Author:
Philippe Manyacka Ma Nyemb, Laboratory of Anatomy and Organogenesis, Faculty of medicine, Gaston Berger University, Saint-Louis, Sénégal, Tel: (+221) 774454313; Email: phil_manyacka@yahoo.fr
Keywords
Subclavian artery; Collateral
branches; Anatomical variations; Flap
surgery
Abstract
Introduction: The arteries of the posterior cervical triangle (lateral cervical region) are frequently used for flap design in plastic and reconstructive surgery. In particular, the musculocutaneous flaps, such as the flap of the lower trapezius and the dorsal scapular flap, are based on the integrity and functional availability of the dorsal scapular artery. Likewise, the cervico-dorsal and cervico-scapular flaps are based on the superficial cervical artery. We can assume that the mode of birth of these arteries - and the possibility of their origin directly from the subclavian artery - will have consequences on their vascular dynamics. These consequences can result in good or bad viability of the irrigated flaps. The objective of the present study was to highlight the birth modalities of the subclavian artery branches
Material and Methods: Dissection was performed in 58 anatomical regions from 32 non-formalin fixed cadavers. The cadavers had no history of surgery or deformity in the areas targeted for dissection (supraclavicular and dorsal regions). They were embalmed using a glycerin-rich, formalin-free solution to preserve tissue suppleness.
Results: The average age of the donors was 72.32 years (range, 34–90) and there were 21 males and 11 females. We find some similarities, with a predominance for types D (Cervico-scapular trunk from the thyrocervical trunk: 28%), A (Separate origin of superficial cervical, dorsal scapular, and suprascapular arteries: 19%), and C (Cervico-dorsal trunk from the subclavian artery: 15%).
Conclusion: There are many anatomical variations concerning the birth modalities of the collateral branches of the subclavian artery. Surgical teams should consider these variations when exploring the region of the lateral triangle of the neck.
Citation
Manyacka Ma Nyemb P, Fontaine C, Demondion X, Demeulaere M, Descamps F and Ndoye JM. Branching Pattern of Collateral Branches of the Subclavian Artery. SM J Clin Anat. 2018; 2(1): 1006
Introduction
The subclavian artery is divided into 3 parts by its relations with the anterior scalene muscle: a pre-scalene part medially located with respect to the medial margin of the anterior scalene muscle, a retro-scalenic part located behind the anterior scalene muscle, and a post-scalene part laterally located with respect to the lateral edge of the anterior scalene muscle [1]. The collateral branches of the subclavian artery can originate from each of these portions, with multiple and varied birth modalities. These anatomical variations that may occur all along the length of the subclavian artery have potential clinical and surgical implications [2]. In plastic and reconstructive surgery, several muscular and musculocutaneous flaps of the cranial part of the thorax depend on the collateral branches of the subclavian artery from a vascular point of view [2]. The surgery of such flaps must therefore also be considered from the point of view of the anatomical variations found on the collateral branches of the subclavian artery. The objective of the present study is to highlight the birth modalities of the subclavian artery branches and their respective frequencies, using a series of cadaveric dissections
Surgical Anatomy
The left and right subclavian arteries essentially supply the posterior part of the encephalon, the spinal cord and the upper limb. The right subclavian artery arises from the brachiocephalic arterial trunk, and the left subclavian artery arises from the aortic arch. Each subclavian artery end under the middle of the clavicle, to become the axillary artery. The left subclavian artery is 3 cm longer than the right one. Their diameter is about 9 to 10 mm [1].
The right subclavian artery arises behind the sternoclavicular joint and moves laterally, describing a curve whose concavity rests on the pleural dome and the first rib (Figure 1).

Figure 1: Dissection of the right subclavian artery on an anterior view
The left subclavian artery originates from the aortic arch and ascends vertically, then follows the same curvilinear path as its counterpart. The 2 subclavian arteries pass between the anterior and middle scalene muscles in the interscalenic space (Figure 2)

Figure 2: Interscalenic space [1]. 1, ventral branch of C5; 2, middle scalene muscle; 3, ventral branch of C6; 4, ventral branch of C7 and middle trunk; 5, dorsal scapular artery; 6, lower trunk; 7, posterior scalene muscle; 8, subclavian artery; 9, vertebral artery; 10, ventral branch of C3; 11, ventral branch of C4; 12, anterior scalene muscle; 13, upper trunk; 14, phrenic nerve; 15, vagus nerve; 16, subclavian vein.
so they are described in 3 parts: pre-scalenic, inter-scalenic and post-scalenic. The subclavian arteries give several branches (Figure 3)

Figure 3: The subclavian artery and its branches on a lateral view [1]. 1, vertebral artery; 2, ascending cervical artery; 3, inferior thyroid artery; 4, thyro-cervical trunk; 5, internal mammary artery; 6, deep cervical artery; 7, transverse artery of the neck; 8, costo-cervical trunk; 9, supreme intercostal artery; 10, dorsal scapular artery; 11, suprascapular artery.
the vertebral artery, the internal mammary artery, the thyro-cervical trunk, the costo-cervical trunk, the dorsal scapular artery [1]
The vertebral artery vascularizes the posterior part of the brain and the cranial part of the spinal cord; its diameter is about 4 mm. It originates from the upper face of the subclavian artery and runs vertically to the level of the C6 vertebra (Figure 3). It enters the transverse foramina of C6 and crosses from bottom to top all transverse foramina of the overlying vertebrae. It leaves the transverse foramen of the atlas and describes a curve that embraces the posterior side of its lateral face. Finally, it crosses the posterior atlanto-occipital membrane and enters the foramen magnum to merge with its opposite counterpart and form the basilar artery [1].
The internal mammary artery originates from the posterior side of the pre-scalenic portion of the subclavian artery and descends behind the first six costal cartilages (Figure 3). It is divided at the level of the 6th intercostal space with 2 arteries: the musculo-phrenic artery and the superior epigastric artery [1].
The thyro-cervical trunk is 9 mm long; it originates from the pre scalenic part of the subclavian artery (Figure 3). It runs vertically and usually divides into 4 branches: the lower thyroid, cervical ascending, transverse cervical and supra-scapular arteries. The lower thyroid artery runs vertically in front of the medial margin of the anterior scalene muscle to the level of the carotid tubercle. It joins the lower end of the lobe of the thyroid gland. The ascending cervical artery ascends along the transverse processes of the cervical vertebrae between the anterior scalene muscle and the longus capitis muscle [1]. The transverse artery of the neck runs laterally, then passes in front of the anterior scalene muscle and passes through the brachial plexus. It is divided at the anterior edge of the levator scapulae muscle in 2 arteries: the superficial cervical artery and the dorsal scapular artery. The suprascapular artery passes the anterior scalene muscle and then behind the clavicle, in front of the brachial plexus.
The costo-cervical trunk is born from the posterior side of the pre-scalenic part of the subclavian artery (Figure 3), at the same level as the internal mammary artery. It heads back to the neck of the 1st rib and divides into 2 branches: the deep cervical and the supreme intercostal arteries. The deep cervical artery usually runs backwards between the transverse process of C7 and the neck of the 1st rib. Then it climbs between the semispinalis muscles of the head and neck. The supreme intercostal artery descends between the pleura and the first 3 ribs [1].
The dorsal scapular artery originates from the post-scalenic portion of the subclavian artery (Figures 3 and 4).

Figure 4: The subclavian artery and its branches in posterior view [1]. 1, suprascapular artery and nerve; 2, subclavian artery; 3, dorsal scapular artery; 4, levator scapulae muscle; 5, small rhomboid muscle; 6, large rhomboid muscle; 7, circumflex artery of the scapula; 8, thoraco-dorsal artery; 9, teres major muscle; 10, supraspinatus muscle; 11, infraspinatus muscle; 12, teres minor muscle; 13, deltoid muscle; 14, axillary nerve and posterior circumflex artery of the humerus; 15, radial nerve and deep artery of the arm.
It runs laterally and crosses the trunks of the brachial plexus at the level of the middle scalene muscle. Then it goes down to the trapezius muscle with the dorsal scapular nerve
Material and Methods
Dissection was performed in 58 anatomical regions from 32 non formalin fixed cadavers. The average age of the donors was 72.32 years (range, 34–90) and there were 21 males and 11 females. The cadavers had no history of surgery or deformity in the areas targeted for dissection (supraclavicular and dorsal regions). They were embalmed using a glycerin-rich, formalin-free solution to preserve tissue suppleness.
For the first stage, the cadaver was placed in dorsal decubitus and the posterior triangle (lateral cervical region) was approached to remove the clavicle. The subclavian artery and its collateral arteries were dissected, identified and marked. The collateral branches of the subclavian artery were injected with a solution containing a mixture of gelatin, methylene blue and iron powder. The cadaver was then refrozen for 24 hours.
In the second stage, the cadaver was thawed out at room temperature. The dissection of the subclavian artery collateral branches was conducted until complete exposure of their path.
Results
After our dissections, we found several birth modalities (See Figure 5 and Table 1),

Figure 5: Illustration of the birth modes of the collateral branches on a right subclavian artery [2]. Labels: C, superficial cervical artery; D, dorsal scapular artery; S, suprascapular artery; A, ascending cervical artery; T, inferior thyroid artery; V, vertebral artery; IT, internal thoracic artery; CDT, cervico-dorsal trunk; CST, cervico-scapular trunk; DST, dorso-scapular trunk; CDST, cervico dorso-scapular trunk. Type A: Separate origin of superficial cervical, dorsal scapular, and suprascapular arteries (19%). Type B: Cervico-dorsal trunk from the thyrocervical trunk (10%). Type C: Cervico-dorsal trunk from the subclavian artery (15%). Type D: Cervico-scapular trunk from the thyro cervical trunk (28%). Type E: Cervico-scapular trunk from the subclavian artery (none). Type F: Dorso-scapular trunk from the subclavian artery (none). Type G: Cervico-dorso-scapular trunk from the thyrocervical trunk (7%). Type H: Cervico-dorso-scapular trunk from the subclavian artery (12%). Type I: Cervico-dorso-scapular trunk from the internal thoracic artery (9%).
Table 1: Modalities of birth of collateral branches of the subclavian artery in 58 dissected specimens.
| Specimen number by order |
|
|
Modalities of birth of the collateral branches of the subclavian artery |
| of dissection |
Age |
Sex |
(Types A-F/ See Fig. 5) |
| 1 |
67 |
F |
I |
| 2 |
88 |
H |
A |
| 3 |
89 |
H |
H |
| 4 |
90 |
F |
G |
| 5 |
75 |
F |
D |
| 6 |
57 |
H |
D |
| 7 |
59 |
H |
B |
| 8 |
62 |
H |
C |
| 9 |
69 |
F |
A |
| 10 |
65 |
H |
D |
| 11 |
78 |
H |
D |
| 12 |
73 |
H |
H |
| 13 |
72 |
H |
C |
| 14 |
88 |
F |
A |
| 15 |
63 |
H |
A |
| 16 |
72 |
H |
I |
| 17 |
77 |
F |
H |
| 18 |
58 |
F |
A |
| 19 |
87 |
F |
B |
| 20 |
63 |
H |
C |
| 21 |
64 |
H |
I |
| 22 |
74 |
H |
D |
| 23 |
65 |
H |
D |
| 24 |
75 |
F |
D |
| 25 |
90 |
H |
A |
| 26 |
72 |
F |
C |
| 27 |
88 |
F |
B |
| 28 |
69 |
H |
G |
| 29 |
67 |
H |
I |
| 30 |
78 |
H |
A |
| 31 |
64 |
H |
H |
| 32 |
75 |
H |
A |
| 33 |
75 |
H |
D |
| 34 |
63 |
F |
C |
| 35 |
81 |
H |
G |
| 36 |
78 |
H |
A |
| 37 |
85 |
H |
D |
| 38 |
85 |
H |
D |
| 39 |
75 |
F |
D |
| 40 |
81 |
H |
A |
| 41 |
87 |
F |
B |
| 42 |
67 |
F |
C |
| 43 |
82 |
H |
G |
| 44 |
85 |
H |
D |
| 45 |
69 |
F |
A |
| 46 |
77 |
F |
I |
| 47 |
73 |
H |
D |
| 48 |
80 |
H |
H |
| 49 |
80 |
H |
H |
| 50 |
79 |
H |
C |
| 51 |
69 |
F |
B |
| 52 |
34 |
H |
C |
| 53 |
34 |
H |
H |
| 54 |
57 |
H |
D |
| 55 |
61 |
F |
D |
| 56 |
47 |
F |
B |
| 57 |
77 |
H |
C |
| 58 |
81 |
H |
D |
as reported by Weiglein et al. [2] in their study
Discussion
The arteries of the posterior cervical triangle (lateral cervical region) are frequently used for flap design in plastic and reconstructive surgery. In particular, the musculocutaneous flaps, such as the flap of the lower trapezius [3-5] and the dorsal scapular flap [6], are based on the integrity and functional availability of the dorsal scapular artery. Likewise, the cervico-dorsal and cervico-scapular flaps [7] are based on the superficial cervical artery. We can assume that the mode of birth of these arteries - and the possibility of their origin directly from the subclavian artery - will have consequences on their vascular dynamics. These consequences can result in good or bad viability of the irrigated flaps. In their work Weiglein et al. [2] report that the birth modalities of the collateral branches of the subclavian artery are predominant for types A, G, D, B and C (Figures 5 and 6). In our work, we find some similarities, with predominance for types D, A, C, H and B (Figures 5 and 6)

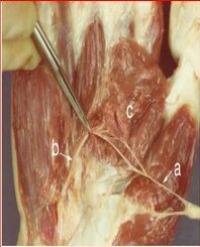
Figure 6: Dissection of a right subclavian artery: cervico-dorsal trunk from the thyro-cervical trunk (Type B, see Figure 5)
Bean [8] reported that branches of the subclavian artery differ in their origins, both on the right and on the left sides. Type A (according to his own classification) or its equivalent was more frequent on the left side, and type B predominated on the right side. In his results it appears that in black race subjects he mostly found a type B and a type A in caucasian subjects
Variations in the birth of the collateral branches of the subclavian artery have a high incidence in Black race subjects according to DeGaris [9,10]. His publications report variations in 40% of Caucasian subjects, and in 75% of American Black subjects. Indeed, in colour races in general and in the black race in particular, several authors have reported a higher frequency of anatomical variations concerning muscular, skeletal and visceral structures. This important prevalence of anatomical variations in colour races is believed to be due to miscegenation.
Huelke [11] also studied the arteries of the lateral triangle of the neck. According to him, the dorsal scapular artery originates from the second or third part of the subclavian artery in 67% of cases. It constitutes a branch of the transverse artery of the neck in only 30% of cases. The transverse artery of the neck was born from the thyro cervical trunk in the majority of cases (77.5%). It is formed as a direct branch (37.1%) or a common trunk (40.4%) with the suprascapular artery. The transverse artery of the neck arises from the dorsal scapular artery in 20% of cases [11]. The combined results of our work show that in 21 cases, the dorsal scapular artery and the transverse artery of the neck originated from a common trunk stemming from the subclavian artery; in 27 cases, the dorsal scapular artery arises directly from the subclavian artery while the transverse artery of the neck comes from the thyro-cervical trunk; and in 10 cases, the dorsal scapular artery and the transverse artery of the neck are both collateral branches of the thyro-cervical trunk.
The anatomical abnormalities found on the collateral branches of the subclavian artery can be explained by the embryological development of this region [12]. The two congenital factors that influence the development of these branches are the ability of the blood to follow the longitudinal channels offering the least resistance, and the tension on the vessels resulting from the caudal displacement of the heart and the aorta.
Congdon [13] described the development of subclavian arteries from the 7th pair of dorsal arteries. He found that the tension on the distal portion of the right aortic arch is at the origin of the formation of the proximal portion of the right subclavian artery from that portion of the aortic arch and from the 4th right dorsal segmental artery. In case of failure of the obliteration of the distal part of the 7th dorsal segmental artery, degeneration of the proximal part occurs. This degeneration results in abnormal origins of the right subclavian artery from the arch of the aorta or the descending aorta.
Thus, because of the caudal displacement of the aorta, the proximal portions of the segmental arteries are exposed to longitudinal stresses and curvatures resulting in a delay in blood circulation. This may contribute to abnormal connections between the longitudinal channels and the subclavian artery or the aortic arch [13-15].
Conclusion
There are many anatomical variations concerning the birth modalities of the collateral branches of the subclavian artery. These variations concern the whole length of the subclavian artery, from its origin to its end. During any vascular surgery of the lateral triangle region of the neck, these anatomical variations must be taken into account in order to limit circulatory complications
References
1. Kamina P. Anatomie Clinique, Tome 2, Tête-cou-dos. 3ème edition. Paris: Maloine. 2006.
2. Weiglein AH, Moriggl B, Schalk C, Künzel KH, Müller U. Arteries in the posterior cervical triangle in man. Clinical Anatomy. 2005; 18: 553-557.
3. Maruyama Y, Nakajima H, Fujino T, Koda E. The definition of cutaneous vascular territories over the back using selective angiography and the intra arterial injection of prostaglandin E1: some observations on the use of the lower trapezius myocutaneous flap. Br J Plast Surg. 1981; 34: 157-161.
4. Netterville JL. Wood DE. The lower trapezius flap: vascular anatomy and surgical technique. Arch Otolaryngol Head Neck Surg. 1991; 117: 73-76.
5. Weiglein AH, Haas F, Pierer G. Anatomic basis of the lower trapezius musculocutaneous flap. Surgical and Radiologic Anatomy. 1996; 18: 257 261.
6. Angrigiani C, Grilli D, Karanas YL, Longaker MT, Sharma S. The dorsal scapular island flap: an alternative for head, neck, and chest reconstruction. Plast Reconstr Surg. 2003; 111: 67-78.
7. Hyakusoku H, Yoshida H, Okubo M, et al. Superficial cervical artery skin f laps. Plast Reconstr Surg. 1990; 86: 33-38.
8. Bean RB. Observations on a study of the subclavian artery in man. Amer J Anat. 1905; 4: 303.
9. DeGaris CF. Patterns of branching of the subclavian artery in white and negro stocks. American Journal of Physical Anthropology. 1924; 7: 95-107.
10. DeGaris CF. Modes of origin of the subclavian artery in whites and negroes, with report of a case of anomalous right subclavian artery. The Anatomical Record. 1923; 26: 235-240.
11. Huelke DF. A study of the transverse cervical and dorsal scapular arteries. The Anatomical Record. 1958; 132: 233-245.
12. Vorster W, Du Plooy PT, Meiring JH. Abnormal origin of internal thoracic and vertebral arteries. Clin Anat. 1998; 11: 33-37.
13. Congdon ED. Transformation of the Aortic-Arch System during the Development of the Human Embryo. Contributions to embryology. 1922; 14: 47.
14. Bergman RA. Compendium of human anatomic variation: text, atlas, and world literature. Urban &Schwarzenberg. 1988.
15. Nizanowski C, Noczyński L, Suder E. Variability of the origin of ramifications of the subclavian artery in humans (studies on the Polish population). Folia morphol. 1982; 41: 281-294.