Case Report | Volume 10 - Issue 1 | Article DOI : https://dx.doi.org/10.36876/smcr.1102
Download PDF
Ming Wu1, Shelley Schwartz2, Steven C. Cramer3*, and Michael Su3
1Department of Medicine, Robert Wood Johnson Medical School, USA
2Department of Internal Medicine, UCLA, USA
3Deparment of Neurology, University of California, Los Angeles; and California Rehabilitation Institute, USA
Corresponding Author:
Steven C. Cramer, Department of Neurology, David Geffen School of Medicine at UCLA, 710 Westwood Plaza, Reed C239, Los Angeles, CA 90095-1769, USA, Tel: (424) 522-7273
Abstract
Cognitive deficits can impact functional outcomes as well as the efficacy of rehabilitation therapy after stroke, but these must be understood in the context of the specific cognitive impairments. We describe here functional improvement during admission to an inpatient rehabilitation facility (IRF) in a patient with an uncommon form of cognitive abnormality, Alice in Wonderland Syndrome (AIWS), which is characterized by visual and other perceptual distortions. The course of this syndrome in the context of inpatient rehabilitation therapy has not been previously described. A 52-year-old male with an acute ischemic infarct involving the left (dominant) occipital, posterior parietal, and posterior temporal lobes received intensive rehabilitation therapy in an IRF setting. The patient reported complete resolution of his AIWS symptoms by day 14 of his IRF admission (day 22 after stroke onset), with daily assessments showing steady gains in his self-care score. Current results suggest that intensive rehabilitation therapy can be provided in the setting of AIWS, and that functional recovery can occur in the presence of AIWS symptoms.
Keywords
Stroke; Rehabilitation; Cognitive deficits; Therapy; Recovery
Citation
Wu M, Schwartz S, Cramer SC, Su M (2024) Going Down the Rabbit Hole: Functional Recovery from Alice in Wonderland Syndrome during Rehabilitation Therapy. A Case Report. SM J Case Rep 10: 3.
INTRODUCTION
Cognitive deficits are common after stroke and can impact functional outcomes as well as the efficacy of rehabilitation therapy [1,2]. These issues vary according to the specific nature and the severity of cognitive deficits, underscoring the importance of characterizing such deficits in individual patients. We report here a patient with Alice in Wonderland Syndrome (AIWS), which is associated with a particular set of cognitive deficits, which consist of distortion of personal perception of somatosensory and visual input, as well as distortion of the perception of time.
AIWS has been described across a wide range of diagnostic categories, including migraine, temporal lobe epilepsy, brain tumors, CNS infection, psychoactive drugs, and stroke [3-5]. The long-term outcome of AIWS varies widely across these conditions [3]. Despite the potential for long term adverse effects, there is no known treatment for AIWS [3,5]. We report here a patient with AIWS due to an acute ischemic stroke in whom symptoms resolved and functional status improved during admission to an inpatient rehabilitation facility (IRF).
CASE PRESENTATION
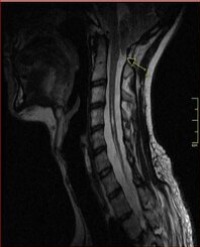
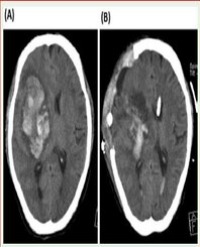
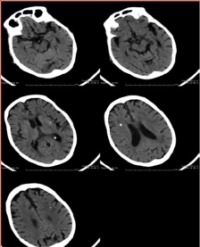
A 52-year-old right-handed male presented to a local emergency room with vision changes, right-sided weakness, and confusion. He also noted blurry vision for one week. Past medical history included hypertension, hyperlipidemia, coronary artery disease treated with percutaneous coronary intervention, heart failure with preserved ejection fraction, end stage renal disease on peritoneal dialysis, type 2 diabetes mellitus, and obstructive sleep apnea. Magnetic resonance imaging (MRI) of the brain revealed an acute ischemic infarct involving the left occipital, posterior parietal, and posterior temporal lobes (Figure 1A). Over the next four days, the patient continued to complain of right visual field loss with floaters. The acute care hospital course was complicated by sepsis due to Clostridium difficile and an isolated witnessed seizure (semiology not documented) that occurred six days after admission, for which he was started on oral levetiracetam. The patient became encephalopathic. An electroencephalogram (EEG) captured an electrographic seizure originating from the left frontal pole.
Over the next few days, the patient noted slight improvement in his blurry vision and right visual field deficits. However, as his sensorium improved, the patient reported various visual disturbances that were distressful and frustrating to him. Examples included seeing text and body parts enlarge and shrink, objects suddenly appearing much closer or further to him while he was ambulating, persisting trails after movement in his vision, and illusory movements in his peripheral vision. He also reported bizarre visual hallucinations such as grass growing out of his sink, as well as a landscape in the corner of his hospital room. He retained insight into all of these hallucinations. The distortions were paroxysmal, typically lasting about 30-60 seconds, and there were no identifiable triggers. He denied diplopia or any associated changes in his visual acuity. He also did not report headaches, changes in his perception of time, or unusual bodily sensations.
His general examination was unremarkable. His neurological examination was notable for rare word-finding difficulties but otherwise fluent speech output. He had full visual fields, intact pupillary reflexes, impaired color vision perception in his right eye (as tested by Ishihara color plates), normal extraocular muscle movements, and no visual neglect. Strength testing revealed mild weakness in his right leg, 4+ out of 5 on the Medical Research Council Scale. The remainder of his neurological examination was normal.
On day 8 of the acute care hospital admission, the patient was transferred to an IRF. During the IRF admission, he received a total of 798 minutes of physical therapy (PT), 470 minutes of speech language pathology therapy (SLP), and 631 minutes of occupational therapy (OT), with at least eight sessions (each 45-60 minutes in duration) that were focused on his visual symptoms. The OT and SLP used a multitude of therapeutic strategies, including redirection techniques, matching and ID tasks, visual scanning, and perceptual tasks (e.g., reading a grocery list and identifying items and prices on a grocery ad), puzzles, Q-Bitz visual perception/problem solving tasks, and word finding activities. The patient was additionally referred to neuro-optometry and neuro-ophthalmology.
A neuropsychology consult suggested that the patient’s repeated focusing on his deficits were contributing to anxiety symptoms. The patient was given recommendations including diaphragmatic/box breathing, grounding techniques, and distress tolerance strategies to manage his anxiety. He was further encouraged to engage in mindfulness, meditation, and the hospital’s yoga group. Finally, neuropsychology advised the use of cognitive remediation and frequent reorientation to aid in the patient’s overt awareness of his symptoms.
Over two weeks, he reported a decrease in frequency of his visual symptoms, with complete resolution of all AIWS-related symptoms 22 days after stroke onset, all while he was still an inpatient in the IRF. He remained on levetiracetam and did not have further seizures. Vision testing at the end of his rehab course was unchanged. On day 16 of admission to the rehabilitation facility, 24 days after stroke onset, the patient was discharged home. Over a 2-year follow-up period, there were no recurrences of his visual disturbances.
The patient’s functional ability was assessed each day via the 24-Section GG scores using standard testing procedures [6]. Scores improved over time in both the self-care score group (a sum of seven tests, range = 7-42) and the mobility score group (a sum of 17 tests, range = 15-90). Higher scores indicate better function and independence. A linear regression fit was significant for self-care (r=0.64, p=0.0075; Figure 1B) but not for mobility (r=0.29, p=0.28).
DISCUSSION
Cognitive impairments are common after stroke. Such deficits may persist for years and are associated with poorer long-term survival and higher disability [2]. Many types of cognitive deficits can occur post-stroke, and to understand how these can impact functional outcomes, it becomes necessary to characterize the specific type of cognitive impairment that is present. Here we describe cognitive deficits in a patient with AIWS as well as their resolution over time, in parallel with improvements in self-care.
AIWS is a neurological disorder associated with distortion of personal perception of somatosensory and visual input, as well as perception of time. Patients with AIWS generally report two classes of symptomatology: metamorphopsias (visual distortions, including micropsia, macropsia, and teleopsia) and aschematias (altered perceptions of self and time) [3]. The long-term outcome in patients with AIWS is highly variable. Most patients with AIWS have symptoms that are self-limited and improve over time, although in some cases symptoms persist for years [3]. There is no established treatment for AIWS [3,5]. The incidence of AIWS is difficult to ascertain, as epidemiologic data are scarce and there are no clear universally accepted diagnostic criteria, well-established pathophysiologic mechanisms, or representations in standard diagnostic manuals [3,4,7].
AIWS has been described in the context of many conditions, including migraine, epilepsy, CNS infections, and cerebrovascular disease (both ischemic and hemorrhagic lesions) [8]. In terms of disease pathogenesis, it has been postulated that the local irritative activity produces an imbalance between primary and secondary cerebral cortices, resulting in electrical phenomena such as epileptic seizures and cortical spreading depression. AIWS has previously been associated with a frontal lobe epileptic seizure [4]; the current patient had a seizure localized by EEG to the left frontal lobe, distant from the region of acute ischemic injury (Figure 1A).

Current treatment of AIWS is focused on supportive care combined with treatment of any underlying condition that has been identified [3,5]. Case reports describe novel approaches that aim to reduce symptoms. For example, one case report examined the effects of 15 sessions of 1 Hz repetitive transcranial magnetic stimulation (rTMS), each 20-minutes in duration, directed at the left temporoparietal junction in a patient with schizoaffective disorder. The patient noted reduced symptoms within the first week and complete resolution by the second week, with no side effects. The patient’s visual distortions returned eight months later and went into remission after 5 additional rTMS treatment sessions [9].
We report here the resolution of symptoms in an AIWS patient in the context of inpatient stroke rehabilitation therapy. The patient spent 16 days in an IRF receiving rehabilitation therapy for his ischemic stroke, during which he received daily sessions of PT, OT, and SLP. The patient experienced significant improvement in self-care as well as complete resolution of his AIWS symptoms. This is an uncontrolled case report, but results indicate that provision of intensive rehabilitation therapy is feasible in the setting of AIWS. We postulate that this rehabilitation therapy might have potentially helped with resolution of AIWS symptoms, a possibility that warrants further study in a controlled trial, though stabilization of cortical irritability and seizures with levetiracetam may have also been contributory. Current results also that presence of AIWS symptoms does not necessarily prevent functional recovery after stroke (Figure 1B).
DATA AVAILABILITY
Data from this case report will be shared upon reasonable request.
CONFLICTS OF INTEREST
Dr. Cramer serves as a consultant for Abbvie, Constant Therapeutics, BrainQ, Myomo, MicroTransponder, Neurolutions, Panaxium, NeuExcell, Elevian, Helius, Omniscient, Brainsgate, Nervgen, Battelle, and TRCare.
REFERENCES
1. Poynter L, Kwan J, Vassallo M. How does cognitive impairment impact on functional improvement following the rehabilitation of elderly patients? Int J Clin Pract. 2013; 67: 811-815.
2. Winstein CJ, Stein J, Arena R, Bates B, Cherney LR, Cramer SC, et al. Guidelines for Adult Stroke Rehabilitation and Recovery: A Guideline
for Healthcare Professionals From the American Heart Association/ American Stroke Association. Stroke. 2016; 47: e98-e169.
3. Blom JD. Alice in Wonderland syndrome: A systematic review. Neurol Clin Pract. 2016; 6: 259-270.
4. Mastria G, Mancini V, Vigano A, Di Piero V. Alice in Wonderland Syndrome: A Clinical and Pathophysiological Review. Biomed Res Int. 2016; 2016: 8243145.
5. Weissenstein A, Luchter E, Bittmann MA. Alice in Wonderland syndrome: A rare neurological manifestation with microscopy in a 6-year-old child. J Pediatr Neurosci. 2014; 9: 303-304.
6. Centers for Medicare & Medicaid Services. Inpatient Rehabilitation Facility PPS.
7. Domenico C, Lavano S, Chirchiglia P. Neurophysiology of a double aura in migraine and Alice in wonderland syndrome: Is there a link?.Neurology, Psychiatry Brain Res. 2019; 32: 1-3.
8. Lanska DJ, Lanska JR. The Alice-in-Wonderland Syndrome. Front Neurol Neurosci. 2018; 42: 142-150.
9. Blom JD, Looijestijn J, Goekoop R, Diederen KM, Rijkaart AM, Slotema CW, et al. Treatment of Alice in Wonderland syndrome and verbal auditory hallucinations using repetitive transcranial magnetic stimulation: a case report with fMRI findings. Psychopathology. 2011; 44: 337-344.