Background: At the 13th St Gallen International Breast Cancer Conference in 2013, a new definition of luminal A-like and luminal B-like breast cancer was proposed, involving the expression of Estrogen Receptor (ER), Progesterone Receptor (PgR), and Ki-67. We examined the rate of concordance between the risk groups using the Oncotype DX Recurrence Score (RS) and the previous and newly proposed luminal subtypes with the standardized Ki-67 assessment.
Method: The relationship between a previously and newly proposed, immunohistochemically defined luminal A and B subtype with the Oncotype DX RS of 41 cases of T1-2 N0-1 M0 (ER positive, HER2 negative) breast cancer was assessed. We first classified the patients into the previously defined luminal A and B subtypes, according to the level of Ki-67 as either “low” (<14%) or “high” (≥14%), as assessed by local pathologists. Next, to consider the necessity for standardizing Ki-67 measurement methods, we re-examined Ki-67 with a central review. By introducing PgR positivity (≥20%), we classified these patients to newly proposed luminal subtypes and compared them with the risk groups stratified by Oncotype DX RS.
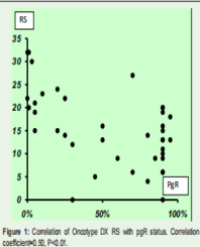
Results: In the previously proposed luminal subtypes, the concordance rate between luminal A and the low RS category was 76.5% according to local pathologists and 90.1% by central review, whereas the rate between luminal B and the intermediate to high RS category was 46.7% and 45.8%, respectively. In newly proposed luminal subtypes, the concordance rate between luminal A and low RS category was 100% and between the luminal B and intermediate to high RS category was 53.6%.
Conclusion: Although this study was based on a retrospective chart review of a small sample size, the newly proposed luminal subtypes, including addition of PgR positivity, appeared to improve the precision of selecting patients with intermediate to high RS categories.
Yoshio Mizuno1*, Hiromi Fuchikami1 , Naoko Takeda1,2, Junichi Yamada3 , Yuko Inoue2 , Hiroshi Seto4 and Kazuhiko Sato1