Accidental Transplantation of a Deceased Donor Kidney with a Large Calculus: Case Review and Management
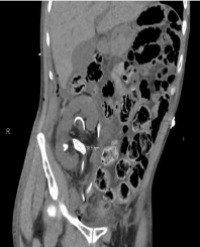
Historically, the presence of stones in a donor kidney has been a contraindication to kidney use for transplantation. However, favorable experiences transplanting living donor kidneys with isolated stones as well as successful management of de novo stone formation following living or deceased donor kidney transplantation have provided insights regarding the benefits and risks of this strategy. The limited supply of available donor kidneys has led to a reexamination of donor selection criteria to meet demand. This reevaluation is also influenced by medical advancements that have allowed for the safe management of allograft kidney stones without compromising outcomes. Herein we report the accidental transplantation of a kidney with a large pre-existing calculus from an otherwise acceptable deceased donor. Based on literature review and given the benefits of kidney transplantation versus dialysis in the setting of prolonged waiting times, expansion of the donor pool to include kidneys with large or multiple stones may be a feasible option to improve utilization and access without necessarily compromising subsequent outcomes.
Keywords: Donor-Gifted Stone; Donor Selection; Kidney Nonuse; Percutaneous Nephrolithotomy; Urolithiasis
Abbreviations: CT: Computerized Tomography; eGFR: Estimated Glomerular Filtration Rate; KDPI: Kidney Donor Profile Index.
Jigish B. Vyas1, Randy K. Casals2, Colin E. Kleinguetl2, Bradley M. Swinson3, Christopher J. Webb1, Alan C. Farney1 and Robert Stratta1*
