Silent Giant Left Atrial Myxoma: Letter to Editor
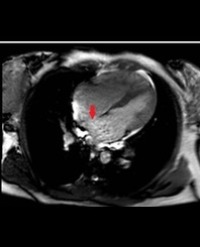
A 33-year-old woman was referred to cardiology assessment 3 months after the delivery of her f irst child because of fatigue. Her past medical history was insignificant. She had no other history of cardiovascular disease. Her physical examination findings were unremarkable. Her laboratory results, including ECG were within normal limits. An echocardiogram showed a notched, highly mobile, 13.0x4.0 cm huge left atrial myxoma covered with thrombi, which nearly fills the left atrial chamber with prolapsed of the tumor mass across the mitral annulus into the left ventricle in diastole (Figure1A-B). Neither significant mitral regurgitation nor mitral stenosis was seen. There was no evidence for patent foramen ovale or other intra-cardiac shunts by color flow Doppler. She subsequently underwent an uneventful surgical removal of the mass at another cardiac surgery center.
Mustafa Yurtdaş1*, Nesim Aladağ1, Mahmut Özdemir1, Yalin Tolga Yaylali2, Yemlihan Ceylan1 and Çağın Zaim3