Research Article | Volume 2 - Issue 1 | Article DOI :
Download PDF
Kevin King*, Philip Blumenfeld, Jacob Y Shin, George Tolekidis and Aidnag Diaz
Department of Radiation Oncology, Rush Medical Center, USA
Corresponding Author:
Kevin King, Department of Radiation Oncology, Rush Medical Center,1653 W Congress Pkwy, Chicago, IL 60612, USA, Tel: 6302406173
Keywords
Glioblastoma; Glioma; Recurrent; SRS; fSRT; Salvage therapy; Outcomes; Patterns of failure
Abstract
High-Grade Gliomas (HGG) are the most common and aggressive primary brain malignancies in adults. Fractionated Stereotactic Radiotherapy (fSRT) and Stereotactic Radiotherapy (SRS) have emerged as a novel technique to deliver high doses of RT in the recurrent setting with aim for durable local control and potential overall survival benefit. This study evaluated the patterns of recurrence, prognostic indicators as well as the efficacy of treatment in patients with recurrent HGG treated by fSRT or SRS. Favorable outcomes were observed in patients treated with fSRT and SRS as salvage therapy. The predominant mode of failure post salvage SRS and fSRT remains in-field. Prospective trials are required to better define patient selection, tumor recurrence size, and effective dose regimen.
Citation
King K, Blumenfeld P, Shin JY, Tolekidis G and Diaz A. Fractionated Stereotactic Radiotherapy and Stereotactic Radiosurgery as Salvage Treatment for Recurrent Malignant High-Grade Gliomas. J Radiat Oncol Res. 2018; 2(1): 1003.
Introduction
High-Grade Gliomas (HGG) remain one of the most common and aggressive primary brain malignancies. Glioblastoma Multiforme, the most common HGG, has a relative five-year survival of 0.05%-4.7% providing for a poor prognosis despite modern treatment modalities [1,2]. Standard treatment includes surgical resection, adjuvant chemotherapy, and Radiotherapy (RT) [1,3]. Despite the combination of these treatment approaches, local recurrence remains the main pattern of failure [4-6]. Thus, treatment of these HGG remains a challenge within the field of neuro-oncology.
Fractionated Stereotactic Radiotherapy (fSRT) and Stereotactic Radiosurgery (SRS) have emerged as novel modalities to deliver focused, high-dose RT in the setting of local failure and recurrence with the aim of durable control and an overall survival benefit [2,7-10]. fSRT is able to deliver precise doses to a predetermined target volume while minimizing the risk of radiation-induced side effects by subdividing effective doses [9,11]. Likewise, SRS is able to deliver a higher dose of irradiation to a smaller target volume to focus on the area specifically affected by the malignancy while sparing surrounding normal structures [12-14]. Numerous studies have shown the efficacy of fSRT and SRS within individual institutions [5,11-14]. The overall survival of these studies range between 5.3-10.6 months from time of salvage treatment [15].
The addition of chemotherapy has also shown to be associated with a modest survival benefit for recurrent GBM [16,17]. While most of the studies examined the role of temozolomide or nitrosoureas, a novel therapeutic agent, bevacizumab, has shown promising results [15,18,19]. Bevacizumab acts as a Vascular Endothelial Growth Factor (VEGF) inhibitor and has since replaced temozolomide as the standard of care for disease failure following prior therapy. However, studies have varied on the actual benefit of bevacizumab. The BRAIN trial showed a 43% six-month progression-free survival with the addition of bevacizumab, but did not show any evidence for improved OS [20]. Currently, Radiation Therapy Oncology Group (RTOG) 1205 is examining the effect of bevacizumab alone versus bevacizumab with concurrent re-irradiation for recurrent GBM.
Our study aims to report our experience treating patients with SRS and fSRT for recurrent HGG and to describe the patterns of recurrence, prognostic indicators and efficacy of treatment in this cohort of patients.
Methods and Materials
A retrospective chart review was performed under approval by the Institutional Review Board at XXXX in XXXX. Patients with recurrent HGG or GBM treated with either fSRT or SRS as salvage therapy between 2006 and 2016 at XXXX were identified. Inclusion criteria in the review consisted of histologically confirmed HGG with radiographic evidence of recurrence by Magnetic Resonance Imaging (MRI) after initial conventional treatment and were subsequently treated with salvage SRS or fSRT.
For patients treated with radiosurgery prior to March of 2012, a stereotactic head frame was placed under local anesthesia. Planning simulation CT of the head was performed for each patient and diagnostic MRI scan was subsequently fused. The Planning Target Volume (PTV) consisted of the contrast-enhancing recurrent lesion (gross tumor volume) with a 1-2-mm margin and was delineated by the neurosurgeon and radiation oncologist on the MR images. Treatment was administered on a Varian Trilogy or Varian 21EX linear accelerator. After March 2012, SRS and fSRT were performed on a Varian True Beam STx (Palo Alto, CA) system. Treatments were planned with either the Brain labiPlan(Westchester, IL), Philips Pinnacle (Amsterdam, Netherlands), or Varian Eclipse (Palo Alto, CA) treatment planning system. With SRS, lesions were treated with 1400 to 2200 cGy and for fSRT lesions were treated with 2000 to 3000 cGy. The dose selection and constraints were based upon RTOG9508 guidelines [21] for SRS and the MSKCC protocol described by Gutin et al. for fSRT [22].
Follow up MRI scans were obtained at both 6 weeks and 3 months unless concerning symptoms were clinically present. Brain MRI and neurological status were used to determine efficacy of treatment.
All patients were evaluated by a neuro-oncologist. Twenty-one patients were started on a bevacizumab treatment course of 10 mg/kg every 2 weeks. There was a wide range in treatment time amongst patients (2-79 weeks) determined at the discretion of the neuro-oncologist. “Bevacizumab naïve” patients were patients with no prior history of receiving bevacizumab. “Bevacizumab failures” were defined as those who had previously received bevacizumab with subsequent HGG recurrence. Finally, a subset of patients either never received bevacizumab or received bevacizumab after salvage RT completion.
Primary end points of the analysis included overall survival as well as patterns of failure Post-Salvage Therapy (pST). Overall survival was calculated from primary diagnosis, time of recurrence, time from RT completion and time from pST chemotherapy completion. Time length for OS was rounded to the nearest month by the 15th day mark. All post-treatment MRI images were reviewed by a neuro-radiologist who determined radionecrosis by examining DWI and T2/ FLAIR for progressively developing confluent non-mass-like white matter changes. These areas also exhibited a lower relative cerebral blood volume and lacked novel foci of restricted diffusion, both of which are characteristics of viable tumors. MRI at time of progression was fused to the treatment planning images to determine the location of recurrence. If the recurrence volume was within the 80% Isodose Line (IDL), it was considered as an in-field failure, while those within the 20-80% IDL were designated as marginal, and less than 20% IDL were considered distant recurrences (Figure 1A and 1B).

Figure 1A: Example of T1 MRI with contrast demonstrating salvage SRS treatment plan for recurrent GBM.

Figure 1B: Example of T1 MRI with contrast illustrating post-salvage therapy progression superimposed with original treatment isodose lines indicating distant recurrence.
There were two patients with tertiary relapse in the analysis. Only initial pST recurrence was included in the analysis of this study.
T-test and Chi-squared test were employed in Microsoft Excel 2010 and SPSS 22.0 for data analysis. The Kaplan-Meier method was used for survival analysis.
Results
Patient characteristics are shown in Table 1. Thirty-one patients with GBM (71.0%) or HGG (29.0%), mainly grade III astrocytoma, were identified. Of the patients with a histologically confirmed GBM and available molecular analysis, twelve were considered to have a primary GBM (85.7%) based off of IDH1 mutation status and two were considered to have a secondary GBM (14.3%) [23]. Eighteen patients were male (66.7%) and thirteen were female (41.9%) with twenty-three having a documented Karfonsky Performance Score (KPS) greater than or equal to seventy (88.0%) at time of initial diagnosis. The median age at diagnosis was fifty-six with a range of twenty-seven to eighty-four. Twenty-five of the patients receiving treatment were Caucasian (80.6%), one was African American (3.2%), two were Hispanic (6.5%), and three were Asian American (9.7%).
Table 1: Patient characteristics (N=31) for those treated with either SRS or fSRT as a salvage treatment option for recurrent high-grade gliomas.
| |
|
SRS |
fSRT |
Total |
| Gender |
Male |
8 |
10 |
18 (66.7%) |
| |
Female |
4 |
9 |
13 (41.9%) |
| Age @ dx |
Years |
56.5 |
56.5 |
56.5 (27-84) |
| Race |
White |
9 |
16 |
25 (80.6%) |
| |
Black |
1 |
0 |
1 (3.2%) |
| |
Hispanic |
2 |
0 |
2 (6.5%) |
| |
Asian |
0 |
3 |
3 (9.7%) |
| KPS |
>70 |
10 |
13 |
23 (88%) |
| Med. Primary Radiation |
Gy |
59.7 |
60 |
60 (52.5-60) |
| Med Time from RT to |
Months |
16 |
9 |
11 (0-63) |
| Progression |
| Primary Dx |
GBM |
10 |
12 |
22 (71.0%) |
| |
Primary GBM |
3 |
9 |
12 |
| |
Secondary |
1 |
1 |
2 |
| GBM |
| |
HGG |
2 |
7 |
9 (29.0%) |
All of the patients underwent surgical resection at the time of initial diagnosis. All of the patients received a full course of RT after primary diagnosis. The median primary radiation dose was 60 Gy. The median time from RT to time of progression was eleven months with a range of zero to sixty-three months. Specifically, the median time of progression of the patients who were treated with SRS was sixteen months and of the patients treated with fSRT was nine months.
All patients were either treated with SRS or fSRT as a salvage therapy at time of initial reoccurrence. Twelve of the patients received SRS (38.8%) and nineteen received fSRT (61.2%) as seen in Table 2. Patients being treated with SRS received a median dose of 19 Gy given in a single fractionation while those treated with fSRT were given a median dose of 5.75 Gy/fraction over five fractionations providing for a total median dose of 19 Gy and 28.75 Gy respectively. Radionecrosis occurred in four of the patients (12.9%).
Table 2: Summary of survival analysis, radionecrosis, and patterns of failure for all patients treated with SRS or fSRT as salvage treatment for high-grade gliomas.
| |
|
SRS |
fSRT |
Total |
| Median OS (mo.) |
Initial Diagnosis |
31 (8-92) |
25 (13-82) |
27 (8-92) |
| |
Recurrence |
14 (6-37) |
8 (1-42) |
11 (1-37) |
| |
Salvage RT |
12 (6-37) |
6 (1-41) |
10 (1-37) |
| Completion |
| |
Never Receiving Bev |
10 |
16 |
11 |
| |
Bev Failure |
0 |
6 |
6 |
| |
Bev Naïve |
13 |
7 |
9 |
| |
Bev After Salvage RT |
33 |
0 |
33 |
| Radionecrosis (n) |
|
1 (3.2%) |
3 (9.7%) |
4 (12.9%) |
| Patterns of Failure |
In-Field |
2 |
8 |
10 |
| (n) |
| |
Marginal |
0 |
3 |
3 |
| |
Distant |
1 |
2 |
3 |
| |
None |
5 |
6 |
11 |
Seven of the patients (22.6%) had a history of being treated with bevacizumab before salvage therapy and twelve (38.7%) were bevacizumabnaïve. Two patients (6.5%) received bevacizumab after salvage therapy. Ten patients (32.3%) never received bevacizumab at any point during their treatment. The median OS from the time of salvage therapy for patients who failed an initial course of bevacizumab was six months (n=7). Survival for bevacizumab naïve patients was nine months (n=12). Survival for patients who never received a treatment of bevacizumab was eleven months (n=10) and survival for patients receiving bevacizumab pST was thirty-three months (n=2) (Table 2).
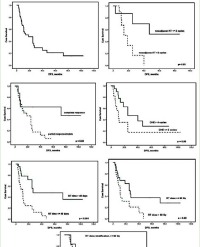
Of those receiving SRS, the median Overall Survival (OS) from the date of initial diagnosis was thirty-one months, from the date of recurrence was fourteen months, from the date of salvage RT completion was twelve months, and from the date of pST chemotherapy completion was seven months. When stratified by PTV, the median OS from date of recurrence was eighteen months for those with PTV ≤0.69 cubic centimeters (cc) and 12 months for those with PTV >0.69 cc (Figure 2). The 2-year overall survival for tumors ≤0.69 cc was 80.0% (±17.9), and >0.69 cc was 50.0% (±25.0) (p=0.183).

Figure 2: Kaplan-Meier overall survival: SRS vs fSRT Stratified by PTV Volume. A: 2-year overall survival (p=0.183), ≤0.69 cc: 80.0% (±17.9), >0.69 cc: 50.0% (±25.0). B: 2-year overall survival (p=0.958), ≤15.91 cc: 63.6% (±14.5), >15.91 cc: 85.7% (±13.2).
For patients treated with fSRT, the median OS from the date of initial diagnosis was twenty-five months, from the date of recurrence was eight months, from the date of salvage RT completion was six months and from the date of pST chemotherapy completion was three months. When stratified by PTV, the median OS from date of recurrence was nine months for those with PTV ≤15.91 cc and sixmonths for those with PTV >15.91 cc (Figure 2). The 2-year overall survival for tumors ≤15.91 cc was 63.6% (±14.5) and >15.91 cc was 85.7% (±13.2) (p=0.958).
Of those receiving SRS with available imaging and dosimetric data, five did not show any known evidence of disease progression, two had in-field recurrence pST, zero had marginal recurrence pST, and one had distant recurrence pST. Of those receiving fSRT with available imaging and dosimetric data, six did not have evidence of progression, eight had in-field recurrence pST, three had marginal recurrence pST and two had distant recurrence pST. Overall, ten of the patients that recurred had in-field recurrence pST (62%), three had marginal recurrence pST (19%) and three had distant recurrence pST (19%) (Figure 3).

Figure 3: Patterns of Failure Post Salvage Therapy. 62% In-Field (n=10), 19% Marginal (n=3), 19% Distant (n=3).
Discussion
Tumor control has become the mainstay in treatment for recurrent HGG indicating a need for salvage therapy. More often than not, these tumors are also unresectable only further complicating a scenario limited by previously failed treatment modalities. Thus, insight into prognostic and predictive indicators of survival is imperative to best select patients for aggressive treatment.
Radiation as an option for recurrent HGG has shown results of OS similar to that of surgical resection with an average of 10-12 months pST [5]. Novel radio-chemotherapeutic approaches have become implicated in possibly extending this outcome [6,12,15,24]. Still, OS has varied by institution leading to the implication that experience and patient specific prognostic indicators could be playing a role in survival. However, these implications cannot be adequately compared due to the overarching selection bias associated with treatment.
Given the small population size of our SRS and fSRT cohorts, no significant associations were found between survival and the numerous variables recorded. However, a number of interesting trends were noted. At our institution, our OS was much higher than currently published data for SRS at 14 months from treatment and comparable for fSRT at 8 months. Patients being treated with fSRT seemed to have a decreased survival compared to SRS, but these results were not statistically significant. Larger tumors are associated with worse outcomes andare more likely to be treated with fSRT due to normal-brain tissue toxicity risks associated with SRS to such a large tumor volume [25,26]. Additionally, SRS patients traditionally are those with better performance status leading to a bias in patient selection. While inferences such as this are common throughout the literature, there is no standardization across studies. Additionally, our study suggested a trend towards improved survival for those patients with smaller tumors being treated with SRS, but this was not statistically significant.
In our fSRT and SRS cohorts, the use of bevacizumab did not play a large beneficial role on median OS from time of salvage RT completion. The majority of fSRTpatients received bevacizumab during their treatment (n=11) whereas the majority of SRS patients were never treated with bevacizumab (n=9). This could be due to the fact that patients chosen for fSRT often had a larger tumor burden and thus would need a more aggressive treatment approach. Patients who had already failed a cycle of bevacizumab had the worst survival at 6 months from salvage RT completion. When comparing RT alone to the bevacizumab naïve patients, there was a decrease in the OS with the addition of bevacizumab (11 months compared to 9 months). Again, this could be due to the difference in patient populations chosen for each individual modality. Patients who received bevacizumab pST had an increased survival of 33 months, but these results are not statistically significant as there were only two patients who had previously been treated with SRS. The use of bevacizumab in our patient population is similar to what was previously reported in the literature [20]. RTOG 1205 is currently examining this relationship in a randomized phase II trial.
Chan et al. previously described a novel method in categorizing patterns of failure for recurrent HGG4. Most of these failures remained within the treatment field suggesting that the addition of whole-brain RT to the previously localized field is unnecessary. While this data examined failure at the time of recurrence, our data examined failure pST. Echoing the results of Chan et al. at the time of recurrence, we found that 62% of the failures still remained in-fieldpST. These results again demonstrate that even in the pST setting, whole brain RT has limited additional benefit and further study is required to determine the cause of local failure.
We were limited in our study by multiple factors. First, there is inherent selection bias by the physician as to which patients would receive SRS versus fSRT as well as the treatment planning process in place. Our population was relatively heterogeneous with regard to adjuvant treatments being given, location of tumor, and pathology of tumor as some of our patients had grade III astrocytomas instead of GBM. Likewise, with a population size of 31 divided between two treatment groups, our data does not have the power to perform any type of multivariate analysis to show true statistical significance. Finally, due to the fact that this was a retrospective study, there was no consistent toxicity assessment recorded to validate the use of radiation therapy in the setting of recurrent HGG. The data provided in this study should be used to guide further clinical questions to better understand treatment of recurrent HGG.
Conclusions
The treatment of HGG continues to remain a challenge for radiation oncologists. There is currently not a standard modality for treatment in the recurrent setting. Favorable outcomes were observed in patients treated with fSRT and SRS as salvage therapy with patients at our institution having increased OS with SRS treatment. Although the sample size was small, there was a trend of improved OS for patients with smaller PTVs with the predominant mode of failure post salvage SRS and fSRT remaining in-field, which is representative of patterns of failure at time of recurrence. Still, prospective trials are required to better define patient selection, tumor recurrence size, and effective dose regimen for the treatment of recurrent HGG.
Acknowledgements
T his research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
1. Ostrom QT, Bauchet L, Davis FG, Deltour I, Fisher JL, Langer CE, et al. The epidemiology of glioma in adults: a state of the science review. Neuro Oncol. 2014; 16: 896-913.
2. Barker FG, Chang SM, Gutin PH, Malec MK, McDermott MW, Prados MD, et al. Survival and functional status after resection of recurrent glioblastoma multiforme. Neurosurgery. 1998; 42: 709-720.
3. Redmond KJ, Mehta M. Stereotactic Radiosurgery for Glioblastoma. Cureus. 2015; 7: 413.
4. Chan JL. Lee SW, Fraass BA, Normolle DP, Greenberg HS, Junck LR, et al. Survival and failure patterns of high-grade gliomas after three-dimensional conformal radiotherapy. J Clin Oncol. 2002; 20: 1635-1642.
5. Combs SE, Thilmann C, Edler L, Debus J, Schulz-Ertner D. Efficacy of fractionated stereotactic reirradiation in recurrent gliomas: long-term results in 172 patients treated in a single institution. J Clin Oncol. 2005; 23: 8863 8869.
6. Shapiro LQ, Beal K, Goenka A, Karimi S, Iwamoto FM, Yamada Y, et al. Patterns of failure after concurrent bevacizumab and hypofractionated stereotactic radiation therapy for recurrent high-grade glioma. Int J Radiat Oncol Biol Phys. 2013; 85: 636-642.
7. Patel M, Siddiqui F, Jin JY, Mikkelsen T, Rosenblum M, Movsas B, et al. Salvage reirradiation for recurrent glioblastoma with radiosurgery: radiographic response and improved survival. J Neurooncol. 2009; 92: 185 191.
8. Yazici G, Cengiz M, Ozyigit G, Eren G, Yildiz F, Akyol F, et al. Hypofractionated stereotactic reirradiation for recurrent glioblastoma. J Neurooncol. 2014; 120: 117-123.
9. Vordermark D, Kölbl O, Ruprecht K, Vince GH, Bratengeier K, Flentje M. Hypofractionated stereotactic re-irradiation: treatment option in recurrent malignant glioma. BMC Cancer. 2005; 5: 55.
10. Bir SC, Connor DE Jr, Ambekar S, Wilden JA, Nanda A. Factors predictive of improved overall survival following stereotactic radiosurgery for recurrent glioblastoma. Neurosurg Rev. 2015; 38: 705-713.
11. Amelio D, Amichetti M. Radiation therapy for the treatment of recurrent glioblastoma: an overview. Cancers (Basel). 2012; 4: 257-280.
12. Clark GM, McDonald AM, Nabors LB, Fathalla-Shaykh H, Han X, Willey CD, et al. Hypofractionated stereotactic radiosurgery with concurrent bevacizumab for recurrent malignant gliomas: the University of Alabama at Birmingham experience. Neurooncol Pract. 2014; 1: 172-177.
13. Elaimy AL, Mackay AR, Lamoreaux WT, Demakas JJ, Fairbanks RK, Cooke BS, et al. Clinical outcomes of gamma knife radiosurgery in the salvage treatment of patients with recurrent high-grade glioma. World Neurosurgery. 2013; 80: 872-878.
14. Imber BS, Kanungo I, Braunstein S, Barani IJ, Fogh SE, Nakamura JL, et al. Indications and Efficacy of Gamma Knife Stereotactic Radiosurgery for Recurrent Glioblastoma: 2 Decades of Institutional Experience. Neurosurgery. 2016.
15. Hasan S, Chen E, Lanciano R, Yang J, Hanlon A, Lamond J, et al. Salvage Fractionated Stereotactic Radiotherapy with or without Chemotherapy and Immunotherapy for Recurrent Glioblastoma Multiforme: A Single Institution Experience. Front.Oncol. 2015; 5: 106.
16. Brandes AA, Pasetto LM, Monfardini S. New drugs in recurrent high grade gliomas. Anticancer Res. 2000; 20: 1913-1920.
17. Khosla D. Concurrent therapy to enhance radiotherapeutic outcomes in glioblastoma. Ann Transl Med. 2016; 4: 54.
18. Vredenburgh JJ, Desjardins A, Herndon JE 2nd, Marcello J, Reardon DA, Quinn JA, et al. Bevacizumab plus irinotecan in recurrent glioblastoma multiforme. J Clin Oncol. 2007; 25: 4722-4729.
19. Kreisl TN, Kim L, Moore K, Duic P, Royce C, Stroud I, et al. Phase II trial of single-agent bevacizumab followed by bevacizumab plus irinotecan at tumor progression in recurrent glioblastoma. J Clin Oncol. 2009; 27: 740-745.
20. Friedman HS, Prados MD, Wen PY, Mikkelsen T, Schiff D, Abrey LE, et al. Bevacizumab alone and in combination with irinotecan in recurrent glioblastoma. J Clin Oncol. 2009; 27: 4733-4740.
21. Andrews DW, Scott CB, Sperduto PW, Flanders AE, Gaspar LE, Schell MC, et al. Whole brain radiation therapy with or without stereotactic radiosurgery boost for patients with one to three brain metastases: phase III results of the RTOG 9508 randomised trial. Lancet. 2004; 363: 1665-1672.
22. Gutin PH, Iwamoto FM, Beal K, Mohile NA, Karimi S, Hou BL, et al. Safety and efficacy of bevacizumab with hypofractionated stereotactic irradiation for recurrent malignant gliomas. Int J Radiat Oncol Biol Phys. 2009; 75: 156-163.
23. Ohgaki H, Kleihues P. The definition of primary and secondary glioblastoma. Clin Cancer Res. 2013; 19: 764-772.
24. Niranjan A, Kano H, Iyer A, Kondziolka D, Flickinger JC, Lunsford LD. Role of adjuvant or salvage radiosurgery in the management of unresected residual or progressive glioblastoma multiforme in the pre-bevacizumab era. J Neurosurg. 2015; 122: 757-765.
25. Minniti G, Clarke E, Lanzetta G, Falchetto Osti MF, Trasimeni G, Bozzao A, et al. Stereotactic radiosurgery for brain metastases: analysis of outcome and risk of brain radionecrosis. Radiat Oncol. 2011; 6: 48.
26. Blonigen BJ, Steinmetz RD, Levin L, Lamba MA, Warnick RE, Breneman JC, et al. Irradiated volume as a predictor of brain radionecrosis after linear accelerator stereotactic radiosurgery. Int J Radiat Oncol Biol Phys. 2010; 77: 996-1001.