Research Article | Volume 2 - Issue 1 | Article DOI :
Download PDF
Mustafa Kandaz1*, Özlem Aynacı2, Alperen Tüysüz3, Emine Canyılmaz1 and Adnan Yöney1
1Department of Radiation Oncology, Karadeniz Technical University, Turkey
2Department of Radiation Oncology, Kanuni Education and Research Hospital, Turkey
3Faculty of Medicine, Karadeniz Technical University, Turkey
Corresponding Author:
Mustafa Kandaz, Karadeniz Technical University, Faculty of Medicine Department of Radiation Oncology, Trabzon/Turkey, Tel: 04623775595
Keywords
Malign Melanoma; Radiotherapy
Abstract
Radiation therapy is used for adjuvant therapy on patients with recurrence or lymphadenectomy in the malignant melanomas. Treatment is used for palliative on metastatic patients. Between 1996 and 2017, 35 patients who received adjuvant radiotherapy and 55 patients who received palliative radiotherapy were retrospectively analyzed. Of the 90 patients included in the study, 56 (62%) were men and 34 (38%) were women. Mean age of patients was 63 years (age range: 22–95 years). For all patients, the overall survival time was 32.23 months (95% CI, 16.8–47.6). As an adjuvant therapy, 48 Gy (hypofractionated) radiotherapy was used in 4 patients and 50-66 Gy radiotherapy was used in 31 patients. Overall survival in these patients was 66.14 (95% CI 36.6-95.6) months. Mean metastases that occur in patients is 37.19 months (range: 2-138 months), which are 37 (41%) patients in the brain, 12 (13%) patients in the bone and 6 (7%) patients in the non-regional lymph node metastasis. 20-30 Gy radiotherapy was used for metastasis treatment. Overall survival in brain metastasis, bone metastasis and lymph nodes metastatic patients were 4.22 (95% CI 2.62-5.82), 7.6 (95% CI 1.14-14.05) and 7.33 (95% CI 0-15.03) months respectively. Although, the regional nodal disease can be favorably controlled with lymphadenectomy and radiotherapy, the risk of distant metastases and the risk of disease-related death are high. In addition, metastasis-related symptoms (particularly pain) can be controlled by radiotherapy.
Citation
Kandaz M, Aynac? Ö, Tüysüz A, Cany?lmaz E and Yöney A. Radiotherapy of Malign Melanoma: A Single-Centre Experience from the Eastern Black Sea Region of Turkey. J Radiat Oncol Res. 2018; 2(1): 1004.
Introduction
Malignant Melanoma (MM) is the most aggressive skin cancer, originating from the pigment-producing cells known as melanocytes [1]. MMs typically occur in the skin, but may rarely occur in the eyes, gastrointestinal tract, meninges and various mucosal layers [2]. Despite the fact that MM accounts for only 4% skin cancers, it is the main reason for deaths associated with skin cancers [3]. The increased melanoma incidence is likely due to changes in lifestyle with regard to extreme exposure to sunlight (frequently leading to sunburn) [4].
Melanomas can develop anywhere in the body. Only 25% of MM develops over an existing nevüs, while most of them develop through the skin with normal appearance [5].
The clinical correct recognition, staging and prognostic evaluation of MM are the first essential steps. All lesions will be examined pathologically suspicious for melanoma. The detection of MM in an early stage is highly important, a step of successful treatment. Improved survival rates can be primarily attributed to earlier detection [6].
The primary treatment for melanoma is surgical excision. After surgery, the adjuvant radiotherapy (RT) following lymphadenectomy in node-positive melanoma patients prevents local and regional recurrence.. However, RT as a definitive treatment is often suggested in clear situations, such as medical inoperability, lentiginous melanoma, mucosal melanoma, and ocular melanoma. Furthermore, RT is often used because it is highly effective in providing symptom palliation for metastatic melanoma.
Approximately 90% of MM are diagnosed with non-metastatic. For such tumors, the tumor-specific 10-year survival is 75-85% [2, 33]. The level of invasion (Clark’s level), mitotic rate, ulceration, Vertical tumor thickness (Breslow’s depth), increased age, family history, sex and location (i.e. truncal/head and neck tumors) are evaluated as clinical and histological prognostic factors.
The first location of metastasis is the regional lymph node (LN), followed by skin (transit metastases), lung and liver. The central nervous system metastases occur in nearly half of patients with metastatic melanoma and in 15–20% of these patients. The central nervous system (CNS) is the first site of relapse. The estimated median survival time for patients with CNS metastases is only 2-4 months [7]. The 10-year survival rate is 30-50% for transit metastases and 20-40% for clinically apparent lymph metastases [8].
The purpose of this study is to report the characteristics, treatment modalities and Disease-Free Survival (DFS) and Overall Survival (OS) of patients with MM in the Eastern Black Sea Region.
Materials and Methods
This study was approved by the Ethics Committee at the Karadeniz Technical University Faculty of Medicine, project no: 2018-23. Records of 90 patients with a diagnosis of MM treated at our clinic between 1996 and 2017 were reviewed. Patients’ information about their age, gender, surgical treatment, local recurrence, distant metastases, and survival were recorded. The patients were grouped by treatment modality.
Treatment
Thirty-five patients were included, those who had been diagnosed with neck, axillary or inguinal LN metastases from MMs and were managed with lymphadenectomy and RT, with or without systemic therapy. Having LN extracapsular extension, an LN measuring 3 cm in size, four or more involved LN, or recurrent disease after previous LN dissection alone for the pathologically confirmed disease are features that increase the risk of regional LN recurrence after surgery and represent the indications for radiating most of the patients in this study.
Conventional RT was performed with a total of 50-66 Gray (Gy) RT per day 2 Gy. Hypofractionated RT was performed in 48 Gy of 20 fractions (2.4 Gy per fraction). We performed radiotherapy for symptom palliation in patients with metastatic melanoma. Metastatic patients were treated with 30 Gy of 10 fractions or 20 Gy of 5 fractions.
Follow-up
Patients were clinically examined by their complete blood test at 1, 3, 6 and 12 months after treatment, and then at six month period. The OS was considered as the time between diagnosis and the last control or death date.
Statistical methods
The obtained data were subjected to the statistical analysis by using Statistical Package Of Social Sciences (SPSS) version 16 software. The OS was calculated by using Kaplan–Meier method. The log-rank test was used in analyzing the differences between subgroups. The Cox regression analysis was performed to predict the factors with independent prognostic significance on survival. All tests were considered statistically significant at p<0.05.
Results
Patient characteristics
Of the 90 patients included in the study, 35 patients who received adjuvant RT and 55 patients who received palliative radiotherapy were retrospectively analyzed. Patients’ ages at the time of presentation ranged from 22 to 95 years, with a mean of 63.04 years. 56 (62%) were men and 34 (38%) were women (a female-to-male ratio of 1:1.6). The mean age, 63.26 (range: 22 to 95) years for the women and 62.9 (range: 27 to 92) years for the men.
The primary site was the head and/or neck in 28 (31%) patients, the trunk in 19 (21%), upper extremity in 21 (23%) and lower extremity in 22 (25%).
Twenty-two patients with a primary site underwent wide local excision with macroscopic and microscopic clear surgical margins. The pathologic analysis of the surgical margins was not present in eight patients. In 5 patients the surgical margin was positive. In 20 patients the nodal metastases were identified by sentinel Lymph Node (SLN) biopsy or elective LN dissection. İnvolvement in the LN region, 1 in right neck, 1 in left neck, 1 in the bilateral neck, 6 in the axilla, 7 in left inguinal, 2 in right inguinal and 1 in bilateral inguinal.
Fifteen patients received 50-66 Gy conventional RT in the tumor bed.The 16 patients with positive lymph nodes, 50-66 Gy conventional RT had been delivered to the neck, axilla or inguinal lymph node region and 4 patients had received 48 Gy hypofractionated RT.
Fifty- five patients had metastases at diagnosis instantly, which 37 (41%) patients in the brain, 12 (13%) patients in the bone and 6 (7%) patients in the patients with non-regional lymph nodes metastasis. Also, bone metastasis occurred in eight patients with brain metastases. Metastatic patients had received 20-30 Gy palliative RT. This patients were treated with systemic treatment after RT.
Survival
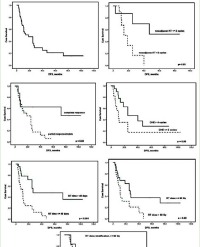
For the thirty-five patients treated with adjuvant RT, the median follow-up period was 42.65 months (range, 3 to 182 months). Local recurrence was seen in three patients (8%) after treatment (range: 8 to 47 months) which two (6%) patients in the inguinal lymph nodes and one patient (2%) in the nasal septum. Four patients with local recurrence underwent systemic treatment. 4 (11%) had distant metastasis during the follow-up after curative treatment. Brain metastasis was seen in two patients, bone metastasis was seen in one patient and non-regional lymph node metastasis was seen in one patient (range: 3 to 13 months). Among the 35 patients treated with adjuvant radiotherapy, the OS time was 67.93 months (95% CI, 37.3–98.5).
There were distant metastases in fifty-five patients. There was distant metastasis at the time of diagnosis in the sixteen patients (29%). For 39 patients (71%), distant metastasis was diagnosed during and after the end of treatment.Mean metastases that occur in patients is 37.19 months (range: 2-138 months), which are 37 (67%) patients in the brain, 12 (22%) patients in the bone and 6 (11%) patients in the non-regional lymph node metastasis.The overall survival in all metastatic patients was 5.74 months (95% CI, 3.76–7.71), the overall survival in brain metastasis, bone metastasis and lymph nodes metastatic patients were 4.22 (95% CI 2.62-5.82), 7.6 (95% CI 1.14-14.05) and 7.33 (95% CI 0-15.03) months respectively.
Discussion
MM is a cancer of the melanocytes that migrate from the neural crest to the epidermis, as well as from the uveal truck, meninges, and ectodermal mucosa. Melanoma is a cancer with the rapid increase incidence worldwide (the melanoma thought to be triggered by ultraviolet rays is more common in areas where exposure to sunlight is high) and a high mortality rate. When diagnosed early, there is a chance of complete cure.
The anatomical origin of skin, which melanomas originated from are different in men and women. In males, while melanoma is frequently in a trunk, it often occurs in the extremities in women and axillary tumors have the worst prognosis [9]. Regardless of the distribution of localizations by sex in our study the primary region is the head and/or neck respectively, while the other regions are the trunk, upper extremity, and lower extremities respectively. Taş et al. reported that skin-derived melanomas were more frequently observed in the extremities with 43.4% unlike our results [10]. İsmail et al., [11] showed that cases of their study was examined according to tumor location, it was seen that the most common site of the tumor was the lower extremity. Also in our country, Karasoy et al. found the most frequent tumor site at head and neck region and lower extremity [12]. In our series, 1/3 of the lesions were located in the head and neck region.
Alfred et al., [13] reported that the mean age of skin melanoma cases was 55.3 years and male/female: 1.19 in an analysis of 84,836 patients diagnosed with melanoma in the US between 1985-1994 in the National Cancer Database registry. In our study patients’ ages were ranged from 22 to 95 years, with a mean of 63 years and the male-female ratio in our patient population was 1/1.6.
The prognosis depends on whether the malignant melanoma is localized, regional, or metastatic at the time of diagnosis [14]. Gender, location, tumor size, depth of invasion, ulcer, staging and sentinel lymph node metastasis were related to patient prognosis as shown by previous studies on the prognostic factors for malignant melanoma [15]. The thickness of Tumor is singlythe most important significative of prognosis, followed by the histologic ulceration and mitotic rate.
Staging of the cutaneous melanoma results in the local, regional and metastatic disease being separated from each other. This difference is directly proportional to survival rates. Stage I and II are defined as early (low risk) and partially early (medium risk) disease respectively. Some features that increase the risk of recurrence of the disease have been observed by the American Joint Committee on Cancer (AJCC) in 1992 and staging systems have been established. In 2000, the staging was re-examined [16]. Distant Metastasis (M1) in both systems representa stage IV, regional lymph node metastasis (N1-3) stage III malignant melanoma.
If the melanoma can be diagnosed and treated at an early stage, it can be cured over 90%, but in advanced stages, survival rates are very low despite promising improvements in treatment. The primary treatment model for cutaneous melanoma is the surgery accompanied by full-thickness excision in order to be able to perform the right staging as well as the treatment [17]. There are 5 randomized controlled trials conducted to date to determine the excisional biopsy limit for melanoma diagnosis.
In a prospective randomized study involving 8 years of the World Health Organization Melanoma Program and 612 patients; in lesions with a depth of invasion of less than 2 mm, excision limits of 3 cm were compared with 1cm excision margin and no difference between disease-free survival and total survival in the study with a mean follow-up of 90 months [18].
In a study of the French Malign Melanoma study group with nine centers located in Europe, 226 patients treated within 5 years were followed up for a mean of 16 years, comparing 2 and 5 cm surgical margins similar to the Swedish group. The 10-year survival and local recurrence rates of the patients were not different in this study [19].
Generally, tumors of 0.5 cm in situ melanomas, 1 cm in 1 mm thin tumors (T1), 1-2 cm in 1-2 mm deep tumors, 2 cm in 2 mm thick tumors (T3 and T4) surgical excision with surgical margin is recommended [20]. In our study, 22 patients (22,4%) with a primary site underwent wide local excision with macroscopic and microscopic clear surgical margins regarding the thickness of tumors. Adjuvant therapy is recommended to reduce risk after surgery in patients at high risk for tumor recurrence.
Regional lymph node metastasis are regarded as a major determinant of the outcome for many malignancies, including melanoma. In addition to tumor thickness over the years, lymph node involvement has become one of the main determinants of the prognosis of the disease. Sentinel lymph node(s) is (are) the first node(s) draining the primary tumor site along the lymphatic pathway. Elective lymph node dissection, lymphedema, nerve damage, wound site problems of any center have clinically, radiologically and pathologically prefer to sample the SLN at the lymph node stage in patients without distant metastases. Lymph node dissection is recommended in cases with a positive SLN sampling [21]. In our study, 20 patients, the nodal metastases were identified by SLN biopsy or elective LN dissection.
RT as a primary treatment is often presented in well-defined cases, such as medical inoperability, lentiginous melanoma, mucosal melanoma and ocular melanoma, although melanoma is a relatively radioresistant tumor [22] and also the adjuvant RT following lymphadenectomy in node-positive melanoma patients prevents local and regional recurrence.
Multiple retrospective studies further defined the role of adjuvant RT. A report from the Sydney Melanoma Unit suggests that the postoperative RT may be an advantage for local control in patients with microscopic positive margins and adverse pathologic features [23]. Karakousis et al. reported that the overall rate of local recurrence was 3.8% [24]. In our study, adjuvant RT was applied to 35 patients. The rate of local recurrence was 8% after treatment which two 6% patients in the inguinal lymph nodes and one patient 2% of the nasal septum. In this study, 35 patients treated with adjuvant radiotherapy, the overall survival time was 67.93 months.
On the other hand, RT is quite effective and widely used in providing symptom palliation for metastatic melanoma [25]. RT was used in the treatment of fifty- five patients with the intent of palliative in our study. The mean survival time of patients with metastatic malignant melanoma is less than a year. Sandru et al. reported that the median overall survival for patients with metastases was about 5.3 months, smaller than that described in large series of patients, in average 7-8 months [26, 27]. The overall survival in all metastatic patients was 5.74 months in our study.
Melanoma is mainly radio-resistant, cell culture studies have shown a broad shoulder in the cell survival curves. This indicates a higher response per fraction, better response and unusual high repair capacity [28]. Radiation Therapy Oncology Group (RTOG) Trial 83-05 was a prospective randomized study comparing hypofractionation to conventional fractionation. The results showed no difference in partial or complete response rates between the two schedules, and the overall response rates were ∼70% [29]. They declared that hypofractionation and conventional fractionation are equally efficacious. In our study, fifteen patients received 50-66 Gy conventional RT and only 4 patients had received 48 Gy hypofractionated RT.
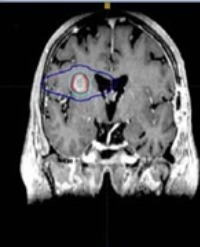
Brain metastasis, a specific form of stage IV melanoma, is one of the most common and difficult to treat complications of melanoma. The percentage of malignant melanomas among cases diagnosed with metastatic intracranial cancer has been reported to be about15.7% [30]. Chason et al., [31] revealed that over 90% incidence of CNS metastases isin their autopsy series. In this series of 122 patients with disseminated malignant melanoma, 46% developed signs and symptoms of CNS disease and 75% had gross evidence of CNS metastases on autopsy. Chiarion- Sileni et al. found that the median survival of melanoma patients with CNS metastases ranges between 2 and 8 months. In our study, the overall survival in brain metastases was 4.2 months.
Skeletal metastases generally occur in patients with widespread metastatic disease and usually represent a late site of recurrence [32]. A large series from Duke University Medical Centre reported BMs in 6.9% of 1677 patients diagnosed with all stages, MM revealed that the mean survival from the diagnosis of bone metastases was about 3.6 months [24]. Cohn-Cedermark et al. reported that the median survival of patients with bones as the first site of metastasis was 2.4 months [33]. In this study, the overall survival in bones was 7.6 months.
References
1. McCourt C, Dolan O, Gormley G. Malignant Melanoma: A pictorial review. Ulster Med. J. 2014; 83: 103-110.
2. Garbe C, Peris K, Hauschild A, Saiag P, Middleton M, Bastholt, et al. Diagnosis and treatment of melanoma. European consensus-based interdisciplinary guideline- Update 2016. European Journal of Cancer. 2016; 63: 201-217.
3. Garbe C, Peris K, Hauschild A, Saiag P, Middleton M, Spatz A, et al. Diagnosis and treatment of melanoma: European consensus-based interdisciplinary guideline. Eur J Cancer. 2010; 46: 270-283.
4. Parlak A, Çayırlı M, Parlak N, Ekinci Ş. Melanoma genel bakış. Konuralp Tıp Dergisi. 2014; 6: 22-27.
5. Mosqueira JR, Gomez E, Bravo F, Vega JD and Soto L. Malignant Melanoma: Case Report and Review of the Literature. Open Access J Trans Med Res. 2017; 1: 00008.
6. Naveed S, Singh G, Hasina Quari H. Subungual Malignant Melanoma: Difficulty in Early Diagnosis. Bangladesh Journal of Medical Science. 2013; 12: 322-324.
7. Douglas JG, Margolin K. The treatment of brain metastases from malignant melanoma. Semin Oncol. 2002; 29: 518-524.
8. Balch CM, Gershenwald JE, Soong SJ, Thompson JF, Atkins MB, Byrd DR, et al. Final version of 2009 AJCC melanoma staging and classification. J Clin Oncol. 2009; 27: 6199-6206.
9. Balch CM, Karakousis C, Mettlin C, Natarajan N, Donegan WL, Smart CR, et al. Management of cutaneous melanoma in the United States. Surg Gyneco lObstet. 1984; 158: 311-318.
10. Tas F, Kurul S, Camlic, H, Topuz, E. Malignant melanoma in Turkey: a single institution’s experience on 475 cases. Jpn J ClinOncol. 2006; 36: 794-799.
11. Şahin İ, Andaç A, Alhan D, Zor F, Öztürk S, Eski M, et al. Malign melanoma olgularının retrospect if değerlendirilmesi. Gülhane Tıp Derg. 2011; 53: 177-181.
12. Karasoy A, Karşıdağ S, Tatlıdere S. Malign melanomada 13 yılda 65 hastadaki deneyimimiz: Retrospektif çalışma. Türk Plastik Rekonstrüktif ve Estetik Cerrahi Dergisi. 2004; 12: 153-157.
13. Chang AE, Karnell LH, Menck HR. The National Cancer Data Base report on cutaneous and noncutaneous melanoma: a summary of 84,836 cases from the past decade. The American College of Surgeons Commission on Cancer and the American Cancer Society. Cancer. 1998; 83: 1664-1678.
14. Plym A, Ullenhag GJ, Breivald M, Lambe M, Berglund A. Plym A, et al. Clinical characteristics, management and survival in young adults diagnosed with malignant melanoma: A population-based cohort study. Acta Oncologica. 2014; 53: 688-696.
15. Russo AE, Ferrau F, Antonelli G, Priolo D, McCubrey JA, Libra M. Malignant melanoma in elderly patients: biological, surgical and medical issues. Expert Rev. Anticancer Ther. 2015; 15: 101-108.
16. Morton DL, Foshag LJ, Hoon DS, Nizze JA, Famatiga E, Wanek LA, et al. Prolongation of survival in metastatic melanoma after specific immunotherapy with a new polivalent melanoma vaccine. Ann Surg. 1992; 216: 463-482.
17. Penegaricano J, Ratanatharathorn V. Cutaneous Malignant Melanoma. Decision Making. Chapter 32, 977-994.
18. Veronesi U, Cascinelli N. Narrow excision (1-cm margin). A safe procedure for thin cutaneous melanoma. Arch Surg. 1991; 126: 438-441.
19. Khayat D, Rixe O, Martin G, Soubrane C, Banzet M, Bazex JA, et al. Surgical margins in cutaneous melanoma (2 cm versus 5 cm forlesionsmeasuringlessthan2.1-mm thick). Cancer. 2003; 97: 1941-1946.
20. Bishop JA, Corrie PG, Evans J, Gore ME, Hall PN, Kirkham N, et al. UK guidelines for the management of cutaneous melanoma. Br J Dermatol. 2002; 146: 7-17.
21. Stebbins WG, Garibyan L, Sober AJ. Sentinel lymph node biopsy and melanoma: 2010 update Part I. J Am Acad Dermatol. 2010; 62: 723-734.
22. Ward W, Farma J. Cutaneous Melanoma Ethiology and Therapy. 2017; 101 120.
23. Stevens G, Thompson JF, Firth I, O’Brien CJ, McCarthy WH, Quinn MJ. Locally advanced melanoma: Results of postoperative hypo fractionated radiation therapy. Cancer. 2000; 88: 88-94.
24. Karakousis CP, Balch CM, Urist MM, Ross MM, Smith TJ, Bartolucci AA. Local recurrence in malignant melanoma: long-term results of the multi institutional randomized surgical trial. Ann Surg Oncol. 1996; 3: 446-452.
25. Fogarty GB, Hong A. Radiation therapy for advanced and metastatic melanoma. J Surg Oncol. 2014; 109: 370-375.
26. Wasif N, Bagaria SP, Ray P, Morton DL. Does metastasectomy improve survival in patients with Stage IV melanoma? A cancer registry analysis of outcomes. J Surg Oncol. 2011; 104: 111-115.
27. Petersen RP, Hanish SI, Haney JC, Miller CC, Burfeind WR Jr, Tyler DS, et al. Improved survival with pulmonary metastasectomy: an analysis of 1720 patients with pulmonary metastatic melanoma. J Thorac Cardio vasc Surg. 2007; 133: 104-110.
28. Rofstad EK. Radiation biology of malignant melanoma. Acta Radiol Oncol. 1986; 25: 1.
29. Sause WT, Cooper JS, Rush S, Ago CT, Cosmatos D, Coughlin CT, et al. Fraction size in external beam radiationtherapy in the treatment of melanoma. Int J Radiat Oncol Biol Phys. 1991; 20: 429-432.
30. Vieth RG, Odom GL. Intra cranial metastases and their neurosurgical treatment. J. Neurosurg. 1965; 23: 375-383.
31. Russo AE, Ferrau F, Antonelli G, Priolo D, McCubrey JA, Libra M, et al. Malignant melanoma in elderly patients: biological, surgical and medical issues. Expert Rev Anticancer Ther. 2015; 15: 101-108.
32. Balch CM, Soong SJ, Shaw HM, Urist MM, McCarthy WH. An analysis of prognostic factors in 8500 patients with cutaneous melanoma. In: Balch CM, Houghton AN, Milton GW, Sober A, Soong SJ, editors. Cutaneous melanoma. Philadelphia: J-B Lippincot; 1992; 165-171.
33. Cohn-Cedermark G, Månsson-Brahme E, Rutqvist LE, Larsson O, Singnomklao T, Ringborg U, et al. Metastatic patterns, clinical outcome, and malignant phenotype in malignant cutaneous melanoma, Acta Oncol. 1999; 38: 549-557.