Research Article | Volume 2 - Issue 1 | Article DOI :
Download PDF
Elif Eda Tiken* and Gülşen Pınar Soydemir
Department of Radiation Oncology, Sadi Konuk Education and Research Hospital, Turkey
Corresponding Author:
Elif Eda Tiken, Department of Radiation Oncology, Sadi Konuk Education and Research Hospital, Turkey, Tel: +905074631919
Keywords
Cervical Cancer; Chemo Radio Therapy; Early Side Effects; Early Response Rates; Local Control
Abstract
The objective of this study is to evaluate early side effects, local control and early response rates of adjuvant or definitive radiotherapy and/or chemo radiotherapy in patients diagnosed with cervical cancer and treated in our clinic. Twenty-one patients who were admitted to our clinic with a diagnosis of stage IB-IVA cervical cancer between January 2017 and November 2018 were included in the study. Adjuvant radiotherapy was performed in 1 patient (5%), adjuvant chemo radiotherapy in 3 patients (14%) and definitive chemo radiotherapy in 17 patients (81%). All patients received intracavitary brachytherapy after radiotherapy. Median follow-up period is 13 months (range: 5-23 months). 12 patients (57%) had a complete response, in 7 patients (33%) had the partial response and in 2 patients (10%) had no response to treatment. 1 (5%) patients who did not respond to the treatment had died. One patient (5%) had lung metastasis, 1 (5%) patients had breast cancer as the second primary. Cystitis and diarrhea were the most common early side effects of radiotherapy. 8 patients (38%) had grade II diarrhea and cystitis and 2 patients (10%) had grade III diarrhea. Nine patients (43%) who received concurrent chemotherapy had grade II-III neutropenia as hematological toxicity. None of the cases had grade IV toxicity. In conclusion, concurrent radio chemotherapy or radiotherapy alone is the preferred treatment modalities in patients with adverse risk factors in stage ≥ IB cervical cancers because of high response rates and acceptable toxicity.
Citation
Tiken EE and Soydemir GP. Adjuvant and Definitive Radiotherapy in Cervical Cancer. J Radiat Oncol Res. 2018; 2(1): 1008.
Introduction
Cervical cancer is the fourth most common cancer in women according to the World Health Organization results (WHO). In 2012 it was 7, 9% of all female cancers [1]. Risk factors include early first intercourse, multiple partners, history of other Sexually Transmitted Diseases (STD)s, high parity, smoking, immunosuppressant, and prenatal Di Ethyl Stilbestrol (DES) exposure for clear cell carcinoma. In 80-90% of cases, the histological type is Squamous Cell Carcinoma (SCC), but the frequency of adenocarcinomas is increasing. Adenocarcinoma of the uterine cervix currently accounts for 16-24% of all cervical carcinomas, while adenosquamous and other histologic subtypes comprise a smaller percentage of patients with cervical cancer. In approximately 90% of patients, there is an association with Human Papilloma Virus (HPV) infection. The prognostic factors of the disease include lymph node metastasis, tumor size, stage, uterine extension and hemoglobin level<10 g/dl. The risk of pelvic node involvement increases with a stage. FIGO clinical staging is used in cervical cancer. Modern imaging methods are also useful [2]. Cystoscopy and sigmoidoscopy are also recommended in locally advanced stage patients and in the presence of symptoms.
Treatment of cervical cancer is selected according to tumor stage. While surgical treatment is used definitively in early-stage disease, Concomitant Chemo Radiation (CRT) followed by Intra Cavitary Brach Therapy (ICRT) is the standard treatment of locally advanced (IB-IV) cervical cancer. Brachytherapy provides a better response by protecting the surrounding normal tissues and increasing dose of the tumor. Adjuvant External Beam Radio Therapy (EBRT) and/or ICRT may be added according to risk factors in patients who underwent definitive surgery. Postoperative pelvic RT indication: Lympho Vascular Space Invasion (LVSI), >1/3 stromal invasion, or >4 cm tumor and postoperative CRT indication: positive margin, positive Lymph Node (LN), or parametrical or greater extension.
We evaluated patients with cervical cancer treated with definitive or postoperative adjuvant concomitant CRT with 40 mg/m2 cisplatin weekly in terms of response, local control and early side effects.
Materials and Methods
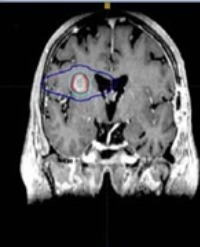
With permission from the Ethics Committee at Health Sciences University Bakırköy Dr. Sadi Konuk Education and Research Hospital we conducted this retrospective clinical study (ethics committee decision number: 2018-253). Twenty-one patients who were admitted to our clinic with a diagnosis of stage IB-IVA cervical cancer between January 2017 and November 2018 were included in the study. The gynecological examination was performed, Pelvic Magnetic Resonance Imaging (MRI) and Positron Emission Tomography (PET-CT) were taken and complete blood count, liver and kidney function tests were evaluated before the treatment. Planning tomography was performed to all patients before external radiotherapy. Fusion of tomography images with pelvic MRI and PET-CT images was performed. Involved in tumor and lymph nodes in T2 weighted MRI was countered as Gross Tumor Volume (GTV). For Clinical Target Volume (CTV), GTV, cervix, uterus, parametrium, vagina, pelvic lymph nodes (par aortic lymphatic’s if involved) were contoured. A Planning Target Volume (PTV) was created by giving 0.5-1 cm margin to CTV.A total of 50.4-60 Gy of EBRT was administered according to the stage of the disease after 45 Gy of the whole pelvis with 1.8Gy fractions daily. At the end of the treatment, all patients underwent gynecological examinations and pelvic MR images were obtained. All patients received ICRT at the external center. The treatment response was evaluated with PET-CT image at 3 months after ICRT. 16 patients received 40 mg/m2 of weekly cisplatin. One patient was not given chemotherapy due to her age. Patients were given weekly controls and side effects were recorded. The patient who was not receiving chemotherapy was excluded from the study.
Statistical Methods
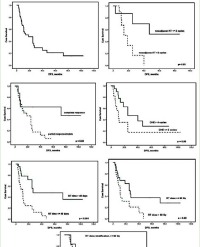
The obtained data were subjected to the statistical analysis by using the SPSS (SPSS for Windows, Version 16.0. Chicago, USA) software. The time of Overall Survival (OS) was calculated from the date of diagnosis to the time of last control or death, while the time of Progression Free Survival (PFS) was calculated from the date of diagnosis to the time of recurrence or metastasis. The relationship between total dose, CRT and clinical results and toxicity were evaluated. Survival rates were calculated using the Kaplan-Meier technique. All significant tests and statistical significance were accepted for a calculated p-value of <0.005.
Results
The mean age of the patients was 53(34-80) years, 14 (67%) were postmenopausal and 7 (33%) were premenopausal. The mean number of pregnancies of the patients was 3 (0-10).6 patients (29%) were stage IB, 3 patients (14%) were IIB, 7 patients (33%) were stage III and 5 patients (24%) were stage IV. 5 (24%) of the cases were adenocarcinoma and 16 (76%) were SCC as histopathologically, Adjuvant EBRT was performed in 1 patient (5%), adjuvant CRT in 3 patients (14%) and definitive CRT in 17 patients (81%). All patients received ICRT after EBRT. Conformal radiotherapy plan was used in 3 patients (14%) and Intensity-Modulated Radio Therapy (IMRT) plan was used in 18 patients (86%).
The RT dose given to 17 (81%) patients was 50, 4 Gy, to 3 (14%) patients 54 Gy and 1 (5%) patient 60 Gy. Within two weeks after RT, in the external center, 18-30Gy ICRT (3-5 fractions x 6 Gy) was applied to the cases. One patient (5%) received 3 cycles, 3 patients (14%) received 4 cycles and 16 patients (76%) received 5 cycles of chemotherapy (Table 1).
Table 1: Patient and treatment features.
| Mean age 53 (34-80) yeras |
n (%) |
| |
Postmenopausal |
14 (67%) |
| Menopause Status |
Premenopausal |
7 (33%) |
| |
Adenocarcinoma |
5 (24%) |
| Histology |
Squamous cell carcinoma |
16 (76%) |
| |
IB |
6 (29%) |
| |
IIB |
3 (14%) |
| |
III |
7 (33%) |
| Stage |
IV |
5 (24%) |
| |
Adjuvant External Beam Radiotherapy |
1 (5%) |
| |
Adjuvant Chemoradiotherapy |
3 (14%) |
| Treatment |
Definitive Chemoradiotherapy |
17 (81%) |
| |
50,4 Gy |
17 (81%) |
| |
54 Gy |
3 (14%) |
| Radiotherapy Dose |
60 Gy |
1 (5%) |
| |
3 cycles |
1 (5%) |
| |
4 cycles |
3 (14%) |
| Chemotherapy |
5 cycles |
16 (76%) |
| |
Alive |
19 (90%) |
| Life Situation |
Dead |
2 (10%) |
Response was evaluated both clinically and radio logically. Response evaluation with clinical evaluation the PET-CT image and clinical evaluation were performed at the 3rd month after treatment. Median follow-up period is 13 months (range: 5-23 months). 12 patients (57%) had a complete response, in 6 patients (29%) had the partial response and in 2 patients (10%) had no response to treatment (Table 2). 1 (5%) patients who did not respond to the treatment had died. The patient who was stage IV and underwent chemotherapy died due to metastasis at 5 months. One patient (5%) developed lung metastasis at 9 months and received chemotherapy and died at the 15th month.1 (5%) patient developed breast cancer as a secondary primary, chemotherapy was applied after surgery. For all patients, the OS time was 12.4±5, 4 months (95% CI, 5-21).-1 year overall survival below and above 60 years of age is 90% and 83% respectively (p=0.808).
Table 2: Response rate.
| Response |
|
Stage |
n (%) |
| |
|
Stage IB |
6 (29%) |
| |
|
Stage IIB |
2 (10%) |
| Complete response |
12 (57%) |
Stage III |
4 (18%) |
| |
|
Stage IIB |
1 (5%) |
| |
|
Stage III |
2 (10%) |
| Partial response |
6 (29%) |
Stage IV |
3 (14%) |
| No response |
2 (10%) |
Stage IV |
2 (10%) |
No patients were discontinued treatment, due to side effect. RT completed in 5-7 weeks and ICRT completed in 1-2 weeks. In all patients, RT and ICRT were completed in 12 weeks.
Cystitis and diarrhea were the most common early side effects of RT.8 patients (38%) had grade II diarrhea and cystitis and 2 patients (10%) had grade III diarrhea. 5 patients (24%) who received concurrent chemotherapy had grade II and 4 patients (9%) grade III neutropenia as hematological toxicity. None of the cases had grade IV toxicity (Table 3). None of the patients had any late side effects.
Table 3: Side effects.
| Side effect |
Grade |
n (%) |
| |
Grade II |
8 (38%) |
| Diarrhea |
Grade III |
2 (10%) |
| Cystitis |
Grade II |
8 (38%) |
| |
Grade II |
5 (24%) |
| Neutropenia |
Grade III |
4 (9%) |
Discussion
Concomitant chemo-irradiation is the standard of care for patients suffering advanced cervical cancer. Adjuvant EBRT and/or ICRT may be added according to risk factors in patients who underwent definitive surgery.
The rate of local control with standard radiotherapy is between 35-90% in stage IB-IV cervical cancer patients. In order to increase the effect of radiotherapy, it has been shown that radiocemotherapy application, especially cisplatin, provides survival advantage in cervical cancers.5-year survival results up to 85-90% with surgery and / or radiotherapy in early stage (stage IA and IB1) cervical cancers [3].
We aim to report the clinical outcome of 21 patients with cervical cancer treated with definitive or postoperative adjuvant concomitant CRT with 40 mg/m2 cisplatin weekly in terms of response, local control and early side effects.
In our study 17 patients (81%) had definitive CRT. 8 patients (57%) had a complete response, in 6 patients (29%) had the partial response and in 2 patients (10%) had no response to treatment. In RTOG 9001 study, subjects were randomized to EBRT + ICRT or RT + ICRT + Cisplatin / 5 FU arms. 8-year OS, disease-free survival increased and reduced local recurrence and distant metastasis with CRT [8,9]. According to a meta-analysis published in 2010, CRT was found to reduce overall survival, progression-free survival, and local recurrence in patients with locally advanced cervical cancer compared with EBRT [10].
In our study, 4 (19%) patients underwent adjuvant EBRT/CRT for postoperative risk factors. No local or distant recurrence was observed in the early period.
In the GOG 92, RTOG 87-06 studies, 277 stage IB patients who had radical hysterectomies were evaluated. Lymphovascular stromal invasion, >1/3 stromal invasion and/or tumor size ≥4 cm are the risk factors and post-op RT addition in patients with ≥ 2 risk factors decreased local and distant recurrence and increased Progression-Free Survival (PFS). No significant difference was found in terms of side effects [4,5]. GOG 109, SWOG 8797, RTOG 91-12 studies evaluated 243 postoperative cases with stage IA2, IB, IIA post-op patients. PFS and overall survival were increased in patients with LN positivity, surgical margin positivity, or parametrium involvement in the arm undergoing postoperative CRT [6,7].
Imaging methods have an important role in the evaluation of patients with cervical cancer. They also help guide treatment decisions. Kusmirek et al., focused on the utility of the current MR imaging and PET/CT protocols in assessing primary tumors and recurrences. It is important to be similar with the MR imaging and PET/CT appearance of the primary tumor and metastasis, as well as the imaging pitfalls. So that an accurate assessment of disease burden is made prior to treatment. [11].
Zhang et al aimed to investigate the importance of perfusion parameters from the peripheral region in predicting the early response to radiotherapy for advanced cervical carcinoma by using Dynamic Contrast-Enhanced (DCE) perfusion Magnetic Resonance Imaging (MRI). They found that perfusion parameters from the peripheral region are more valuable than perfusion parameters from the central region of tumor in predicting the early response to radiotherapy for advanced cervical carcinoma.
Schwarz et al. included 238 cervical cancer cases with PET CT before and after CRT. The complete metabolic response in 173 patients, partial response in 40 patients and progression in 25 patients has been seen [12]. In our study, definitive CRT was applied to 17 patients with locally advanced stage. Eight patients had a complete response, 6 had a partial response, and 2 patients did not respond to treatment according to PET CT images.
There is a debate about whether the histologic type is an independent prognostic factor in cervical cancer. Some series support the prognostic equivalent of cervical adenocarcinoma against SCC, but most have shown a poor prognosis of adenocarcinoma [13]. We evaluated 4 cervical adenocarcinomas patients who were treated. Two of these patients received postoperative CRT because of positive LN and parametrical extension. No recurrence was seen in follow up. However, one of the patients who received definitive CRT had progression and was referred to surgery. The other patient underwent SBRT because ICRT could not be administered.
Acute side effects due to radiotherapy are observed during the treatment or in the first week after the end of treatment. Sub acute side effects are observed within 4-12 weeks after the end of treatment. In the early period after pelvic RT, itching, dry and wet rash, nausea, colitis, cystitis, vaginitis hematological side effects are seen. Treatment-related acute grade 3-4 side effects were seen more frequently in the group receiving concurrent chemo radiotherapy than the group receiving radiotherapy. (p<0,001) [14].
In the study of Özsaran et al., early-stage side effects related to RT were 66.7% and all of them were grade I-II cystitis and diarrhea. Treatment will require a break because of toxicity. None of the cases had grade III-IV toxicity [15]. Radiotherapy for cervical cancer can cause hematological, urogenital and intestinal toxicity, similarly to other combined treatments [16]. Another study showed that, most of the bladder reactions were early reactions appearing during the first three months, and the rate of vesicle and intestinal toxicity was higher after combined therapy with operation and irradiation than after primary radiotherapy [17]. In our study, the early side effects of radiotherapy were cystitis and diarrhea. 8 (38%) patients had grade II diarrhea and cystitis. Grade III diarrhea was seen in 2 (10%) patients. In patients receiving concomitant chemotherapy, grade II-III neutropenia developed as hematological toxicity in 43% (9 patients). None of the cases had grade IV toxicity.
Our study has some limitations. First, as with any retrospective study, unpredictable biases may have influenced our results. Second, the number of patients is low and our follow-up period is short.
There was not any statistical evaluation in terms of response and toxicity with RT dose, stage and other prognostic factors (Hb value, age, co morbidity and tm diameter). Nevertheless, we had a cervical cancer patients treated with the same protocol, and our study may help evaluate of side effects in the presence of chemo radiotherapy protocols.
In conclusion, concurrent CRT is the preferred treatment modalities in patients with adverse risk factors in stage ≥IB cervical cancers because of high response rates and acceptable toxicity.
References
1. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010; 127: 2893-2917.
2. Hansen EK, Roach M. Handbook of Evidence-Based Radiation Oncology. 2010.
3. Lehman M, Thomas G. Is concurrent chemotherapy and radiotherapy the new standard of care for locally advanced cervical cancer? Int J Gynecol Cancer. 2001; 11: 87-99.
4. Sedlis A, Bundy BN, Rotman MZ, Lentz SS, Muderspach LI, Zaino RJ. A Randomized Trial of Pelvic Radiation Therapy versus No Further Therapy in Selected Patients with Stage IB Carcinoma of the Cervix after Radical Hysterectomy and Pelvic Lymphadenectomy: A Gynecologic Oncology Group Study. Gynecol Oncol. 1999; 73: 177-183.
5. Rotman M, Sedlis A, Piedmonte MR, Bundy B, Lentz SS, Muderspach LI, et al. A phase III randomized trial of postoperative pelvic irradiation in Stage IB cervical carcinoma with poor prognostic features: follow-up of a gynecologic oncology group study. Int J Radiat Oncol Biol Phys. 2006; 65: 169-176.
6. Peters WA, Liu PY, Barrett RJ, Stock RJ, Monk BJ, Berek JS, et al. Concurrent Chemotherapy and Pelvic Radiation Therapy Compared With Pelvic Radiation Therapy Alone as Adjuvant Therapy After Radical Surgery in High-Risk Early-Stage Cancer of the Cervix. J Clin Oncol. 2000; 18: 1606-1613.
7. Monk BJ, Wang J, Im S, Stock RJ, Peters WA, Liu PY, et al. Rethinking the use of radiation and chemotherapy after radical hysterectomy: a clinical-pathologic analysis of a Gynecologic Oncology Group/Southwest Oncology Group/Radiation Therapy Oncology Group trial. Gynecol Oncol. 2005; 96: 721-728.
8. Morris M, Eifel PJ, Lu J, Grigsby PW, Levenback C, Stevens RE, et al. Pelvic Radiation with Concurrent Chemotherapy Compared with Pelvic and Para-Aortic Radiation for High-Risk Cervical Cancer. N Engl J Med. 1999; 340: 1137-1143.
9. Eifel PJ, Winter K, Morris M, Levenback C, Grigsby PW, Cooper J, et al. Pelvic Irradiation With Concurrent Chemotherapy Versus Pelvic and Para-Aortic Irradiation for High-Risk Cervical Cancer: An Update of Radiation Therapy Oncology Group Trial (RTOG) 90-01. J Clin Oncol. 2004; 22: 872-880.
10. Chemoradiotherapy for Cervical Cancer Meta-analysis Collaboration (CCCMAC). Reducing uncertainties about the effects of chemoradiotherapy for cervical cancer: individual patient data meta-analysis. Cochrane Database Syst Rev. 2010; CD008285.
11. Kusmirek J, Robbins J, Allen H, Barroilhet L, Anderson B, Sadowski EA. PET/ CT and MRI in the imaging assessment of cervical cancer. Abdom Imaging. 2015; 40: 2486-2511.
12. Schwarz JK, Siegel BA, Dehdashti F, Grigsby PW. Metabolic Response on Post-therapy FDG-PET Predicts Patterns of Failure After Radiotherapy for Cervical Cancer. Int J Radiat Oncol. 2012; 83: 185-190.
13. Kastritis E, Bamias A, Efstathiou E, Gika D, Bozas G, Zorzou P, et al. The outcome of advanced or recurrent non-squamous carcinoma of the uterine cervix after platinum-based combination chemotherapy. Gynecol Oncol. 2005; 99: 376-382.
14. Zeng SY, Li LY, Shu KY, Pan M, Li HP, Luo B. Concurrent chemoradiotherapy versus radiotherapy in advanced cervical carcinoma. Ai Zheng. 2008; 27: 942-946.
15. Souhami L, Seymour R, Roman TN, Stanimir GW, Trudeau M, Clark BG, et al. Weekly cisplatin plus external beam radiotherapy and high dose rate brachytherapy in patients locally advanced carcinoma of the cervix. Int Radiat Biol Phys. 1993; 27: 871-878.
16. Póti Z, Mayer A. Current methods of chemoradiotherapy for locally advanced cervical cancer. Options for reduction of side-effects. Orv Hetil. 2013; 154: 803-809.
17. Böttcher HD, Schütz J, Mathei B. Side effects of the treatment of cervix cancer. Strahlentherapie. 1983; 159: 334-343.