Research Article | Volume 3 - Issue 1 | Article DOI :
Download PDF
Gülşen Pınar Soydemir1 and Mustafa Kandaz2*
1Health Sciences University Bak?rköy, Dr. Sadi Konuk Education and Research Hospital
2Department of Radiation Oncology, Karadeniz Technical University, Turkey
Corresponding Author:
Mustafa Kandaz, Department of Radiation Oncology, Karadeniz Technical University, Trabzon/Turkey, Tel: +905327332909
Keywords
Nasal Cavity and Paranasal Sinus Tumors; Radiotherapy; Side Effects; Overall Survival
Abstract
Nasal cavity and paranasal sinus tumors constitute 3-5% of the upper respiratory tract tumors, 0.2-0.8% of all tumors. Tumors are located approximately 40-50% in the nasal cavity, 30-40% in the maxillary sinus, 10% in the ethmoid and frontal sinuses and 5% in the sphenoid sinuses. Sixty Two patients who were admitted to our clinic with a diagnosis Nasal cavity and paranasal sinus tumors between January 1997 and December 2018 were included in the study. There were 28 (44%) females and 34 (55%) males, for a ratio of 1/1.2. Median age at presentation was 59.4 (range 32 to 87) years. The mean overall survival 59.7± 7 (95% Confidence Interval (CI), 41.3-79.6) months and the median overall survival 38 ± 7 (95% CI, 24.4-49.6) months. The -1, -3 and -5 year overall survival rates were 72.2 %, 51.4 % and 34.6% respectively. The mean disease-free survival 77.4± 8 (95% CI, 51.4-86.1) months and the median disease-free survival 36± 8 (95% CI, 7.65-78.5) months. The -1,-3 and-5 year DFS rates were 69.8%, 49.1% and 39.9% respectively. On Univariate analysis, the OS was significantly better with female sex (p<0.005), < 50 age (p<0.021), T stage (p<0.0001), the absence of lymph node involvement (p<0.0001). In conclusion, PNS/NC is a rare group of cancers. Surgical resection followed by PORT is an effective treatment. RT increases tumor control rate. Local recurrence was the main common cause of failure followed by distant metastasis and regional relapse of the lesions.
Citation
Soydemir GP and Kandaz M. Clinical Outcomes in Nasal Cavity and Paranasal Sinus Tumors: A Single Institution Experience from the Eastern Black Sea Region of Turkey. J Radiat Oncol Res. 2019; 3(1): 1009.
Introduction
Nasal Cavity and Paranasal Sinus Tumors (PNS/NC) constitute 3-5% of the upper respiratory tract tumors, 0.2-0.8% of all tumors [1]. The female-to-male ratio is 1/1.8 [2]. 51.6% of these tumors are squamous cell carcinoma (SCC), 12.6% adenocarcinoma, 6.2% adenoid cystic carcinoma, 6% melanoma and 3.1% undifferentiated carcinoma. The others are lymphoma, plasmacytoma, esthesioneuroblastoma and sarcomas [3,4]. Most of the tumors occur between the ages of 50-70. Sinonasal cancers are more common in carpenters, timber workers and nickel workers.
Tumors are located approximately 40-50% in the nasal cavity, 30-40% in the maxillary sinus, 10% in the ethmoid and frontal sinuses and 5% in the sphenoid sinuses. Tumors superior-posterior to Ohngren’s line had a poorer prognosis. Often, the tumor does not cause symptoms without going beyond the anatomical borders of the sinus. Patients often resort to physicians with nonspecific symptoms such as nasal discharge, nasal obstruction, nasal bleeding. This may cause delays in diagnosis up to 6-18 months [5].
The primary treatment modality for patients is respectable tumors after surgery and adjuvant Radiotherapy (RT) or chemoradiotherapy (CRT). Post-operative RT (PORT) is indicated for patients with close or positive margins, Perineural invasion (PNI) and adenoid cystic tumors. The disease is definitive RT or CRT in inoperable patients. Results for patients with clinical PNS/NC tumors are poor with 5 years Overall Survival (OS) 5-65% and 5-year Local Control (LC) 21-78% [6,7]. Nasal vestibule cancers are skin cancers which are important cosmetic aspects. RT is generally preferred for carcinoma of the nasal vestibule due to the better cosmetic outcome, but if localized, can be done with open margins and no cosmetic deformity.
PNS/NC forms a different group due to their relationship with the adjacent anatomical structure and organs, and they generally come in advanced stages. In general, local control was 91% for T1-T2, 65% for T3, 27% for distant metastasis, and 48% for N2. Prognostic factors; histology (if undifferentiated distant metastasis increases), localization, tumor prevalence, age, performance, and if there is nerve invasion, local control is 64% if not 90% if there is nerve invasion, distant metastasis is 32% or 17%. The surgical margin is difficult to obtain if there is head base involvement, nasopharyngeal invasion, sphenoid sinus invasion, cavernous sinus invasion, and radiotherapy should be added.
In this study was to evaluate clinical features and treatment results in patients with PNS/NC cancer treated with surgery and RT at our institution.
Materials and Methods
Patients selection
The study was conducted on 62 patients who were diagnosed with PNS/NC, treated and followed between January 1997 to December 2018 at our clinical. Metastatic patients were excluded from the study. RT or CRT was applied to all patients. The information about patients was accessed with the retrospective analysis of patient files. Loco regional clinical staging was performed using clinical examinations and Computed Tomography (CT) and/or Magnetic Resonance (MR) and/or PET-CT. Distant metastases were detected using CT, Ultra Sono Graphy (USG) and/or MR. Surgical procedure (total or subtotal excision, lymph node dissection) were recorded. Different surgical approaches depended on tumor location, histological characteristic and stage. Ipsilateral neck dissection was performed in patients of high-grade tumors, radiological or clinical evidence of lymph node metastasis or with the risk of lymph node involvement.
Treatment
RT or CRT was performed in locally advanced disease or in the presence of close or positive margins, PNI and adenoid cystic tumors. Ipsilateral neck lymph nodes were irradiated in patients of pathological lymph nodes or, as elective treatment, in high-risk patients. Definitive RT or CRT dose was planned ranged from 66-70 Gy. The total PORT dose was planned ranged from 60 Gy to 66 Gy for negative and positive microscopic surgical bed margins, respectively, and from 50 Gy to 60 Gy for negative and positive nodes with or without extra capsular extension, respectively.
RT was performed with the linear accelerator of 6 MV-energy and with some patients IMRT and some cases with 2-D and/ or 3-D conformal technique. One daily fraction of 1.8 to 2 Gy for 5 days/week was used for all patients. Head and neck mask was used for immobilization, simulation of all therapy phases. When computed tomography-based treatment was planned, an organ at risk contouring and dose prescription and target volume were performing according to the International Commission on Radiation Units (ICRU) 62 guidelines. Radiotherapy-related acute and late mucosa, soft tissue, skin and temporomandibular joint toxicity were commentated according to the Radiation Therapy Oncology Group/ European Organization for Research and Treatment of Cancer (RTOG/EORTC) scoring system. Radiotherapy-related acute and late mucosa, soft tissue, skin and temporomandibular joint toxicity were commentated according to the Radiation Therapy Oncology Group/European Organization for Research and Treatment of Cancer (RTOG/EORTC) scoring system.
Follow-up
Follow-up was performed every 3 months for the first 2 years, every 6 months for the subsequent 3 years, and once a year thereafter. Clinical and radiological examinations were performed for each visit.
Statistical methods
In this study, clinical outcome was evaluated of disease-free and overall survival. DFS was evaluated between the end of Definitive RT/CRT and PORT and the occurrence of local and/or distant recurrence. The association between clinical outcome (distant metastasis and local recurrence) and tumor characteristics (stage, grade, lymph node metastasis, positive surgical margins, extra capsular extension and perineural invasion) were analyzed. Survival rates were calculated using the Kaplan-Meier technique. All significant tests and statistical significance were accepted for a calculated p-value of <0.005.
Results
Patients characteristics
A total of 62 patients of PNS/NC. There were 28 (44%) females and 34 (55%) males, for a ratio of 1/1.2. Median age at presentation was 59.4± 14.6 (range 32 to 87) years. Of the 62 patients, 17 (27%) occurred in <50 years and 45 (73%) in ≥50 years. The most common histology was SCC (62%), adenoid cystic carcinoma (11%), malign melanoma (10%) and sarcoma (9%). The rarer histology was undifferentiated carcinoma (6%), adenocarcinoma (1%) and lymphoma (1%). Pathological T stage: 1 (1%) patients in stage I, 8 (13%) patients in stage II, 23 (37%) patients in stage III, 19 (31%) patients in stage IVa and 11 (18%) patients in stage IVb. 16 (26%) patients had lymph node involvement (9 (15%) patients in N1, 2 (3%) patients in N2a and 5 (8%) patients N2b) (Table 1).
Table 1: Patient characteristics.
| Characteristics |
n |
% |
| Gender |
| Female |
28 |
44 |
| Male |
34 |
55 |
| Age 32-87 (59.4±14.6) |
| <50 |
17 |
27 |
| ≥50 |
45 |
73 |
| Tumor site |
| Nasal cavity |
11 |
18 |
| Nasal vestibule |
16 |
26 |
| Maxillary sinus |
31 |
50 |
| Sphenoid sinus |
3 |
5 |
| Frontal sinus |
1 |
1 |
| Histology |
| Squamous cell carcinoma |
38 |
62 |
| Adenocarcinoma |
1 |
1 |
| Adenoid cystic carcinoma |
7 |
11 |
| Undifferentiated carcinoma |
4 |
6 |
| Malign melanoma |
6 |
10 |
| Sarcoma |
5 |
9 |
| Lymphoma |
1 |
1 |
| T |
| I |
1 |
1 |
| II |
8 |
13 |
| III |
23 |
37 |
| IVa |
19 |
31 |
| IVb |
11 |
18 |
| N |
| N0 |
46 |
74 |
| N1 |
9 |
15 |
| N2a |
2 |
3 |
| N2b |
5 |
8 |
| Surgery |
| Biopsy |
16 |
26 |
| Subtotal |
14 |
22 |
| Total |
32 |
52 |
| Local recurrence |
| No |
40 |
65 |
| Yes |
22 |
35 |
| Distant metastasis |
| No |
44 |
71 |
| Yes |
18 |
29 |
| Final situation |
| Alive |
26 |
42 |
| Exitus |
36 |
58 |
Treatment characteristics
The biopsy was performed in 16 patients (26%). Subtotal excision was performed to 14 (22%) patients and total.
Excision was performed to 32 (52%) patients. 27 (44%) patients underwent unilateral radical neck dissection. All patients were treated with PORT. Radiation dose were given 18 (29%) patients 60 Gy, 28 (45%) patients 66 Gy and 16 (26%) patients 70 Gy. The fractional dose 1.8/2Gy daily. 22 (35%) patients received tumor bed irradiation. 23 (37%) patients were treated with tumor bed and unilateral neck nodal irradiation and 17 (28%) patients were treated with tumor bed and bilateral neck nodal irradiation. 16 (26%) patients underwent concurrent chemotherapy (weekly cisplatin).
Toxicity
Acute toxicity was noted by seeing skin lesions and oral mucositis. 11 (18%) patients had grade I skin lesions, 34 (55%) patients had grade II, 9 (14%) patients had grade III and 8 (13%) patients had grade IV. 14 (23%) patients had grade I oral mucositis, 24 (39%) patients had grade II, 18 (28%) patients had grade III and 6 (10%) patients had grade IV. Acute toxicity was shown in Table 2. None of the patients developed grade 3 and 4 late toxicity of soft tissues, skin or oral mucosa.
Table 2: Toxicity.
| |
Skin lesions |
Oral mucositis |
| n (%) |
n (%) |
| Grade I |
11 (18%) |
14 (23%) |
| Grade II |
34 (55%) |
24 (39%) |
| Grade III |
9 (14%) |
18 (28%) |
| Grade IV |
8 (13%) |
6 (10%) |
Locoregional recurrens and distant metastasis
Median follow-up 64 months (range, 4-250 months). 22 (35%) patients developed loco regional recurrrens (8- 135 months). 16 of the relapse cases were seen in treatment area and 6 of them were in the neighbourhood. The loco regional recurrences cases included, 12 (19%) male and 10 (16%) female, 14 (23%) SCC, 4 (7%) adenoid cystic carcinoma, 2 (3%) undifferentiated carcinoma, 1 (1%) malign melanoma and 1 (1%) sarcoma. After loco regional recurrence was average survival 32 (range, 2-84) months.
18 (29%) patients developed distant metastasis to the brain in 9(14%) patients, bone in 6(10%) patients and lung in 3 (5%) patients. The distant metastasis cases included, 12(19%) male, 6(10%) female, 9(15%) SCC, 4 (6%) malign melanoma, 3 (5%) sarcoma, 2 (3%) adenoid cystic carcinoma, after distant metastasis was average survival 18 (range, 0-104) months.
Survival analysis
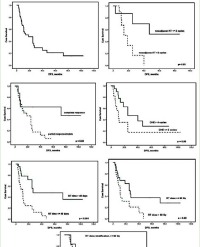
The mean OS 59.7± 7 (95% Confidence Interval [CI], 41.3-79.6) months and the median OS 38 ± 7 (95% CI, 24.4-49.6) months. The -1, -3 and -5 year OS rates were 72.2 %, 51.4 % and 34.6% respectively.
The mean DFS 77.4 ± 8 (95% CI, 51.4-86.1) months and the median DFS 36± 8 (95% CI, 7.65-78.5) months. The -1,-3 and-5 year DFS rates were 69.8%, 49.1% and 39.9% respectively.
On Univariate analysis, the OS was significantly better with female sex (p<0.005), < 50 age (p<0.021), T stage (p<0.0001), the absence of lymph node involvement (p<0.0001).
Discussion
Cancer of the PNS/NC is rare. Tumors are located approximately 40-50% in the nasal cavity, then 30-40% in the maxillary sinus, 10% in the ethmoid and frontal sinuses and 5% in the sphenoid sinuses. The primary treatment modality; if tumors are respectable you should do surgery after adjuvant RT or CRT. RT after surgery is indicated for patients with close or positive margins, PNI and adenoid cystic tumors. If patients have an unrespectable tumor the treatment should be definitive RT or chemo radiotherapy. PNS/NC malignancies continue to be a therapeutic challenge for both tumor control and treatment-related toxicity [6]. RT is usually preferred for carcinoma of the nasal vestibule due to the better cosmetic outcome because of important cosmetic aspects. Nasal and paranasal tumors form a different group due to their relationship with the adjacent anatomical structure and organs, and they generally come in advanced stages. In our study, we aimed; evaluate clinical features and treatment results in patients with PNS/NC cancer treated with surgery and RT at our institution.
The majority of neoplasm’s occurred in the fifth decade of life in previous studies [8,9]. A total of 68 patients were enrolled in the study by Wiegner et al. and the mean age was 63 years [6]. In our study have 62 patient and the median age at presentation was 59.4 (range 32 to 87) years.
A systematic review by Dulguerov et al. evaluated sinonasal tumors over a period of 38 years and found SCC as the most common tumor [10]. In this study, the most common histology was SCC (62%), adenoid cystic carcinoma (11%), malign melanoma (10%) and sarcoma (9%). The rarer histology was undifferentiated carcinoma (6%), adenocarcinoma (1%) and lymphoma (1%). Our findings were consistent with the literature.
In the many studies, acute, radiation-related toxicities included dysphagia, radiodermatitis and nausea/vomiting [11-13]. In this study, acute toxicity was noted by seeing skin lesions and oral mucositis.
Reports from Jiang et al. showed a 5-year recurrence-free survival rate of 51% and a local control rate of 78% in 73 patients with maxillary sinus [14]. Similar results were reported by Roa et al. and Pommier et al. [15.16]. In our study, the mean DFS 77.4 months and the median DFS 36 months. The -1,-3 and-5 year DFS rates were 69.8%, 49.1% and 39.9% respectively.
In the Wiegner’s study [6], sixteen patients (31%) developed distant metastases as a first recurrence, 5 of which were synchronous with a Loco-Regional Failure (LRF). The median time to distant metastases was 9.9 months (range, 2.5-110.3 months). Of the 28 patients with SCC, 13 (46%) experienced LRF at median 7.6 months (range, 2.5-56.9 months) from a time of diagnosis and 10 patients developed distant metastases at median time 7.2 months (range, 2.5-56.9 months). In our study, 18 (29%) patients developed distant metastasis to the brain in 9 (14%) patients, bone in 6 (10%) patients and lung in 3 (5%) patients. The distant metastasis cases included, 12 (19%) male, 6 (10%) female, 9 (15%) SCC, 4 (6%) malign melanoma, 3 (5%) sarcoma, 2 (3%) adenoid cystic carcinoma, after distant metastasis was average survival 18 (range, 0-104) months.
Reports from Bradford et al. showed local control and survival were with a 5-year rate of 62% and 67%, respectively [13]. Results for patients with clinical PNS/NC tumors are poor with 5 years OS 5-65% and 5-year LC 21-78% [6,7] Wiegner et al. study, 2-year OS 66% (6). On Univariate analysis, patients with SCC, more than one sub site involved and residual disease, had significantly worse Locoregional control (LRC) and OS, whereas patients with cribriform plate invasion had worse LRC. Patients who treated with chemotherapy, there was a trend toward worse LRC (p: 0.085), FFDM (p: 0.070), and OS (p: 0.064) on Univariate analysis, which likely reflects the advanced nature of tumors for which chemotherapy was administered. In our study, the mean OS 59.7 months and the median OS 38 months. The -1, -3 and -5 year OS rates were 72.2 %, 51.4 % and 34.6% respectively. On Univariate analysis, the OS was significantly better with female sex (p<0.005), < 50 age (p<0.021), T stage (p<0.0001), the absence of lymph node involvement (p<0.0001).
Our study has some limitations. First, it was a retrospective study conducted at a single center, thereby requiring caution while interpreting the results. Second, this retrospective report includes patients treated in the 22-year period. During this period, the imaging modalities and RT techniques improved, which may have resulted in a selection bias.
Conclusion
PNS/NC is a rare group of cancers. Surgical resection followed by PORT is an effective treatment. RT increases tumor control rate. Local recurrence was the main common cause of failure followed by distant metastasis and regional relapse of the lesions.
References
1. Krespi P, Levine TM. Tumors of the Nose and Paranasal Sinuses. Edited by Paparella MM, Otolaryngology V:III, WB. Saunders Compony. 1991; 1949-1958.
2. Turner JH, Reh DD. Incidence and survival in patients with sinonasal cancer: a historical analysis of population-based data. Head Neck. 2012; 34: 877-885.
3. Harrison DF. A critical evaluation of present-day attitudes to the treatment of antro-ethmoidal cancer. J Otolaryngol. 1982; 11: 148-150.
4. Dirix P, Nuyts S, Geussens Y, Jorissen M, Vander Poorten V, Fossion E, et al. Malignancies of the nasal cavity and paranasal sinuses: Long-term outcome with conventional or three-dimensional conformal radiotherapy. Int J Radiat Oncol Biol Phys. 2007; 69: 1042-1050.
5. Calderón- Garcidueñas L, Delgado R, Calderón-Garcidueñas A, Meneses A, Ruiz LM, De La Garza J, et al. Malignant Neoplasms of the Nasal and Paranasal Sinuses: A Series of 256 Patients in Mexico City and Monterrey. Is air Pollution the Missing Link? Otolaryngol Head Neck Surg. 2000; 122: 499-508.
6. Wiegner EA, Daly ME, Murphy JD, Abelson J, Chapman CH, Chung M, et al. Intensity-modulated radiotherapy for tumors of the nasal cavity and paranasal sinuses: clinical outcomes and patterns of failure. Int J Radiat Oncol Biol Phys. 2012; 83: 243-251.
7. Katz TS, Mendenhall WM, Morris CG, Amdur RJ, Hinerman RW, Villaret DB. Malignant tumors of the nasal cavity and paranasal sinuses. Head Neck. 2002; 24: 821-829.
8. Grau C, Jakobsen MH, Harbo G, Svane- Knudsen V, Wedervang K, Larsen SK, et al. Sino- nasal cancer in Denmark 1982- 1991- a nationwide survey. Acta Oncol. 2001; 40: 19-23.
9. Hoppe BS, Nelson CJ, Gomez DR, Stegman LD, Wu AJ, Wolden SL, et al. Unresectable carcinoma of the paranasal sinuses: Outcomes and toxicities. Int J Radiat Oncol Biol Phys. 2008; 72: 763-769.
10. Dulguerov P, Jacobsen MS, Allal AS, Lehmann W, Calcaterra T. Nasal and paranasal sinus carcinoma: are we making progress? A series of 220 patients and a systematic review. Cancer. 2001; 92: 3012-3029.
11. Hoppe BS, Stegman LD, Zelefsky MJ, Rosenzweig KE, Wolden SL, Patel SG, et al. Treatment of nasal cavity and paranasal sinus cancer with modern radiotherapy techniques in the postoperative setting--the MSKCC experience. Int J Radiat Oncol Biol Phys. 2007; 67: 691-702.
12. Blanco AI, Chao KS, Ozyigit G, Adli M, Thorstad WL, Simpson JR, et al. Carcinoma of paranasal sinuses: Long-term outcomes with radiotherapy. Int J Radiat Oncol Biol Phys. 2004; 59: 51-58.
13. Myers LL, Nussenbaum B, Bradford CR, Teknos TN, Esclamado RM, Wolf GT. Paranasal sinus malignancies: An 18-year single institution experience. Laryngoscope. 2002; 112: 1964-1969.
14. Jiang GL, Ang KK, Peters LJ, Wendt CD, Oswald MJ, Goepfert H. Maxillary sinus carcinomas: Natural history and results of postoperative radiotherapy. Radiother Oncol. 1991; 21: 193-200.
15. Roa WHY, Hazuka MB, Sandler H, Martel MK, Thornton AF, Turrisi A, et al. Results of primary and adjuvant CT-based 3-dimensional radiotherapy for malignant tumors of the paranasal sinuses. Int J Radiat Oncol Biol Phys. 1994; 28: 857-865.
16. Pommier P, Ginestet C, Sunyach M, Zrounba P, Poupart M, Céruse P, et al. Conformal radiotherapy for paranasal sinus and nasal cavity tumors: three- dimensional treatment planning and preliminary results in 40 patients. Int J Radiat Oncol Biol Phys. 2000; 48: 485- 493.