Review Article | Volume 2 - Issue 1 | Article DOI :
Download PDF
Jae Kim*
Department of radiology, University of Central Florida College of Medicine, USA
Corresponding Author:
Jae Kim, University of Central Florida College of Medicine, USA, Tel: +1 407-266-1000
Abstract
Purpose: To report the survival benefit of Radiation Therapy (RT) in Leptomeningeal Carcinomatosis (LMC) patients with different primary cancers and to identify the factors of LMC patients that had survival benefit from Whole Brain Radiation Therapy (WBRT).
Methods and Materials: Systematic literature review was performed. Search terms included ‘Leptomeningeal’, ‘prognostic factors’ and ‘lung’ or ‘breast’. Literatures were included if patient profile was reported. Specifically, age, median survival, diagnosis time line, type of cancer, received treatments, performance score, and systemic disease were sought after. Literatures were excluded if they were a) case reports, b) written in language other than English, or c) not including patient profile.
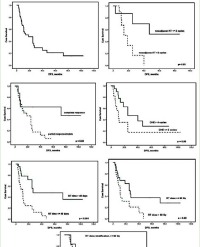
Results: RT treatment has survival benefit for LMC patients with CSF obstruction. For LMC patients with primary breast cancer, 7 studies were found since 1991 that met searching criteria. Factors which would allow breast cancer-caused LMC patients to benefit from WBRT with survival are identified with statistical significance. They include KPS>60, Intrathecal (IT) chemotherapy, systemic therapy, hormonal receptor status and severity of systemic disease. Patients who met aforementioned criteria and received WBRT had longer median survival (17 weeks vs. 11.9weeks, p=0.015). Similarly, 10 studies were found that met searching criteria for Non-Small Cell Lung Cancer (NSCLC) caused LMC. Beneficial factors for NSCLC-caused LMC are identified. They include IT chemotherapy, KPS > 60, and EGFR TKI treatment. Patient who met these criteria had longer median survival when received WBRT (17.6 weeks vs 12.2 weeks, p = 0.0412).
Conclusion: Profiles of LMC patients that can benefit with longer survival by receiving WBRT are identified for breast cancer and NSCLC. Algorithms in identifying such patients are provided.
Citation
Kim J. Examining the Survival benefit of Radiation Therapy on Leptomeningeal Carcinomatosis and Identifying factors Associated with Survival Benefit of WBRT. J Radiat Oncol Res. 2018; 2(1): 1005.
Short Description of this Paper
Today, there is not conclusive data on the survival benefit from radiation therapy for leptomeningeal carcinomatosis patients. Based on published data, the survival benefit of the radiation therapy is reviewed. For breast and NSCLC primary cancers, profiles of LMC patients that experienced survival benefit from Whole Brain Radiation Therapy (WBRT) are identified.
Introduction
Prevalence of Leptomeningeal Carcinomatosis (LMC) is reported to be about 5% of all the patients with cancer [1]. LMC is a detrimental complication of cancer involving the CNS. Without treatment, the median survival from the diagnosis is 4-6 weeks, and with treatment, it is doubled to 8-12 weeks [2-5]. The incidence of LMC has been increasing for the past several decades. Such increase is partially due to a) improved diagnostic modalities, including fine resolution MRI and CT, and b) improved cancer treatment [6]. Paradoxically, with cancer treatment improvement, the risk of LMC increases as the chance for cancer cells to invade the subarachnoid space is increased over time. Today, there is no clear standard of care to treat LMC patients. Due to relatively short median survival, a careful weighing between prolonging lifewhile worsening the quality of life and maintaining the pain-free quality of life without prolonging life needs to be evaluated and discussed with the patient.
As of today, intra-thecal (IT) chemotherapy is the mainstay of the LMC treatment [7,8]. The most common method is using the ommaya reservoir and directly injecting chemotherapeutic agents into the CSF. Many have reported that IT has survival benefit for good risk patient group [9-11]. Radiation Therapy (RT), often used in conjunction with the IT, is used to target symptomatic sites and to relieve mass effect [12]. However, the effectiveness of radiation therapy on overall survival has not been as conclusive as IT treatment. This is partially due to poor prognosis with a short median survival. Such combination along with rapid deterioration of neurologic functions makes randomized trials very challenging. Therefore, RT is mainly considered to be supplemental therapy to IT. For the past decades, multiple retrospective studies were published with conflicting conclusions on the survival benefit of RT. This is mainly because multiple factors contribute to not only clinical progression but also survival. Therefore, it is important to keep such complex dynamics into account when treating/assessing LMC patients.
The purpose of this review is two-fold. The first purpose isto examine the effectiveness of radiation therapy in prolonging the survival of LMC patients.Second isfor different primary cancers; identify constituting factors that would allow LMC patients to have survival benefit when treated with RT. Differentiating factors for breast cancer and lung cancer is crucial as treatment planning including RT changes. Based on identified factors, general algorithm for breast cancer and lung cancer will be devised.
Treatment Overview
LMC management overview
Figure 1 shows the simplified treatment algorithmfor LMC patients.

Figure 1(a): Simplified Algorithm of the LMC treatment.

Figure 1(b): Complete Algorithm of the LMC treatment from NCCN.
Such algorithm was derived from NCCN guideline [13] shown in detail in Figure 2.

Figure 2: CSF Flow Abnormality Correction with RT and Survival Benefit.
Once the diagnosis of LMC is made, the patient is further stratified into either poor-risk or good-risk groups, as shown. For poor risk groups, the therapy is mainly supportive with palliative therapy. On the other hand, for the good-risk group patients, the goal is to control the cancers by aggressively treating the patients. Treatment goals include improving or stabilizing the neurologic function, improving the quality of life, or prolonging life [14]. Achieving any of the three listed treatment goals would consider such treatment effective. For patients that are receiving WBRT, it is recommended to cover the meningeal space, including the lamina cribrosa and basilar cistern.
CSF flow study, radiation therapy and survival benefit
Before the intra-CSF chemotherapy is started, a CSF flow study is recommended, as shown in Figure 1. As cancerous cells invade the subarachnoid space, they can block the CSF outflow. More than 50% of LMC patients are reported to have CSF Flow Abnormality and as high as 70% has been reported by Grossman et al., [15]. As outflow is disturbed, hydrocephalus develops and Intracranial Pressure (ICP) can be elevated. This explains why more than 50% of LMC patients report headache as their chief complain [16]. More importantly, without normal CSF flow, intra-CSF chemotherapy is not recommended due to the possibility of developing neurotoxicity. Intra-CSF chemotherapy relies on normal CSF flow to be distributed throughout the entire neuraxis. CSF flow obstruction will cause toxic chemo agents to build up within the subarachnoid space, a phenomenon described as ‘protected site effect’ by Glantz et al., [17], and cause more toxicity than benefit.It has been reported that such toxicity affected the survival of the LMC patients [18]. In order to assess CSF flow, either Technetium or Indium-DPTA is used [19]. Once the dye is injected, images are taken in such an order that certain compartments should be clear of dye with the elapse of time. Typically, dyes reach the basilar cisterna, lumbosacral sac, and leave the entire ventricle within 10 minutes, 2 hours, and 24 hours, respectively [15,17,20].
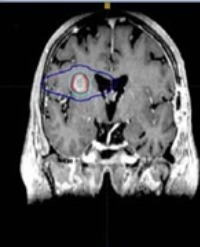
Sensitivity, selectivity and accuracy of CSF flow study is over 99%, whereas detecting flow abnormality using MRI or CT are 60% and 30%, respectively [21]. Once the flow abnormality is detected, focal radiation therapy is used to correct the obstruction [22]. The localized spot is mapped to the brain scan images and radiation is used to treat the obstruction. Glantz et al., [17] and Chamberlain et al., [23] reported survival benefit of RT in LMC patients with flow abnormality. Table 1 summarizes the finding of Glantz et al., [17]. Similar findings have been reported in Grossman et al., [15], and Chamberlain et al., [24].
Table 1: Survival Benefit after CSF Flow correction with RT [17].
| Flow Status |
Survival |
| Normal (N=13) |
6.9 month |
| Abnormal but corrected with RT(N=9) |
13 months |
| Abnormal but uncorrectable (N=9) |
0.7 month |
Radiation therapy hence indirectly provides survival benefit by resolving the obstruction and by allowing effective IT treatment to take place. CSF flow study has been incorporated as part of the LMC treatment guideline. Based on aforementioned findings, the diagnostic and survival algorithm for CSF outflow abnormality can be designed as shown in Figure 2. If the obstruction is corrected, which is shown in the red box from the Figure 2, survival benefit can result.
Breast cancer caused LMC
Breast cancer is the most common solid tumor causing LMC, as it comprises 35% of total solid tumor-based LMC patients [4,6,25]. The breast-cancer-caused LMC rate has been increasing for the last decade mainly due to improvement in breast cancer treatments [1,26]. For breast cancer, the tumor cells directly invading the subarachnoid space is thought to be the most likely cause of dissemination to the meninges [27,28]. The median survival of patients with breast cancer is the highest compared to other primary cancers with 9-30 weeks [10,29,30]. Most common histologic types and biologic subtypes for breast cancer LMC are lobular and triple-negative, respectively [31-33]. This is contrary to the fact that the most common biologic subtype in the general breast cancer population is luminal A [31]. A summary of breast cancer causedLMC is summarized in Tables 1&2.
Table 2: Summarizing the breast cancer type LMC.
| Prevalence (among solid tumor LMC) |
35% |
| Median Survival |
9-30 weeks |
| Most common histologic sub-type |
Lobular |
| Most common biologic sub-type |
Triple-Negative |
| Most common treatment for OS |
IT chemotherapy |
For patients with normal CSF outflow, IT therapy has shown survival benefit for breast cancer caused LMC patients [10,17,29,30,34]. On the other hand, the survival benefit of radiation therapy on breast cancer LMC patients has not been clearly established. In order to study the radiation therapy’s benefit on the overall survival of LMC patients with primary breast cancer, seven papers meeting the searching criteria were found dating from 1991 to 2013. All seven papers discussed radiation therapy as a treatment modality and discussed prognostic factors for LMC patients with breast cancer. Table 3 summarizes the 7 studies and the patient demographics for each study.
Table 3: Summary of breast cancer patients with LMC published in last 20 years.
| |
Boogerd |
Jayson |
Fizazi |
Rudnick |
Gauthier |
De Azevedo |
Niwanski |
| -1991 |
-1994 |
-1996 |
-2007 |
-2010 |
-2011 |
-2013 |
| Number of Patient |
44 |
35 |
68 |
67 |
91 |
60 |
118 |
| Median Age |
57 |
45 |
52 |
49 |
53 |
46 |
49 |
| Median Survival |
12 |
11 |
9.5 |
16 |
14 |
13 |
18 |
| Time from BR to |
38 |
20 |
30 |
27 |
22 |
17.9 |
25 |
| LMC(months) |
| KPS Score> 60 |
N/A |
N/A |
34 |
41 |
N/A |
47 |
80 |
| KPS Score < 60 |
N/A |
N/A |
34 |
26 |
N/A |
12 |
38 |
| Intra-CSF Chemo |
44 |
1 |
41 |
57 |
80 |
41 |
93 |
| Systemic |
20 |
N/A |
42 |
41 |
72 |
13 |
80 |
| WBRT |
22 |
8 |
18 |
33 |
26 |
22 |
66 |
| WBRT benefit on OS |
no |
No |
no |
yes |
No |
No |
Yes |
| Ductal Carcinoma |
N/A |
N/A |
29 |
23 |
52 |
47 |
54 |
| Lobular |
N/A |
N/A |
29 |
22 |
23 |
13 |
32 |
| ER/PR Positive |
17 |
N/A |
13 |
37 |
60 |
28 |
49 |
| Systemic Metastasis |
28 |
N/A |
47 |
29 |
67 |
47 |
57 |
| Most Common |
Bone |
N/A |
bone |
Bone |
bone |
Bone |
Bone |
As can be seen from Table 3, only two studies Rudnick et al., [35] and Niwinski et al., [31] showed survival benefit with the WBRT. These two studieswere compared tothe other five studies. Table 4 shows the comparison of patients who experienced survival benefit with WBRT.
Table 4: Analysis of factors associated with survival benefit of WBRT.
| |
WBRT with Survival Benefit (2 Studies) |
WBRT without Survival Benefit (5 Studies) |
P Value |
| Number of Patients |
185 |
207 |
|
| Median Age |
49 |
50.6 |
0.68 |
| Median Survival(weeks) |
17 |
11.9 |
0.015 |
| Time from BR to |
26 |
25.5 |
0.94 |
| LMC(months) |
| KPS Score > 60 |
121 (65%) |
109 (52%) |
0.01 |
| KPS Score < 60 |
64 (34%) |
97 (46%) |
0.0137 |
| Intra-CSF Chemo |
150 (81%) |
127 (61%) |
<0.0001 |
| Systemic |
121 (65%) |
90 (43%) |
<0.0001 |
| WBRT |
99 (53%) |
70 (33%) |
<0.0001 |
| Ductal Carcinoma |
77 (41%) |
76 (36%) |
0.55 |
| Lobular |
54 (29%) |
42 (20%) |
0.49 |
| ER/PR Positive |
86 (46%) |
41 (19%) |
0.01 |
| Systemic Metastasis |
86 (46%) |
140 (67%) |
<0.0001 |
Statistically significant factors include KPS score, IT chemotherapy, systemic Therapy, hormonal receptor status and severity of systemic disease. Patients that benefited from WBRT had longer median survival with 17 weeks compared to 11.9 weeks with statistical significance (p = 0.015). Patients in the benefited group used more multi-modality treatments, including intra-CSF, systemic, and WBRT (53% vs 33%). Also, the systemic metastatic involvement was substantially lower in the benefitted group (46% vs 67%). Based on Table 4, an algorithm can be created for those who can potentially benefit with longer survival from the radiation therapy (gray box), as shown by Figure 3.

Figure 3: Algorithm for recommending RT therapy for survival benefit based on 7 studies.
Lung cancer caused LMC
Lung cancer is the second most common cause of LMC from solid tumors, comprising about 20% [36]. Without treatment, survival is 4-6 weeks. With treatment, survival can be extended to 16 to 24 weeks [20]. Non-Small Cell Lung Cancer (NSCLC) is the most common cause, constituting >80% of LMC patients [37]. For NSCLC-caused LMC, retrograde flow to the vertebral and para-vertebral venous system with an increased intra-thoracic pressure is believed to be the most common cause of gaining access to the subarachnoid space [27,28]. The most common histologic type is adenocarcinoma, making up more than 85% of lung cancer caused LMC. Current treatment modalities for NSCLC caused LMC includes IT chemotherapy, systemic therapy, RT, and Epidermal growth factor tyrosine kinase inhibitor (EGFR-TKI). Like breast cancer caused LMC, there is no standard treatment protocol as of today. Summary of lung cancer caused LMC is summarized in Table 5.
Table 5: Summarizing the LMC with primary lung cancer.
| Prevalence (among solid tumor LMC) |
20% |
| Median Survival |
12-18 weeks |
| Most common histologic sub-type |
NSCLC |
| Most common cytology |
Adenocarcinoma |
| Most common treatment for OS |
Intra-Thecal |
IT chemotherapy has consistently shown survival benefit for NSCLC caused LMC patients [38-41]. For the past decade, adding EGFR-TKI targeted therapy to the treatment has shown substantial improvement in survival consistently. Nakamura et al., [42] showed patients with EGFR-TKI regiment had median survival of 13 months compared to 4 months of those without EGFR-TKI treatment [42]. Similar results were reported from Morris et al., [39], Lee et al., [40], and Xu et al., [43]. On the other hand, the survival benefit from RT has been reported with inconsistent conclusions. In order to make a more concrete conclusion on the survival benefit of the RT of LMC patients with primary lung cancer, ten papers from 1998 to 2015 were reviewed. All ten papers included WBRT as a treatment modality and discussed prognostic factors for LMC patients with NSCLC. Table 6 summarizes the results.
Table 6: Summary of NSCLC patients with LMC published in last 20 years.
| |
Chamberlain |
Chuang |
Park |
Nakamura |
Morris |
S Lee |
Xu |
Umemura |
Gwak |
Riess |
| -1998 |
-2008 |
-2010 |
-2012 |
-2012 |
-2013 |
-2015 |
-2012 |
-2011 |
-2014 |
| Number of Patients |
32 |
34 |
50 |
67 |
125 |
149 |
108 |
91 |
105 |
30 |
| Median Age |
57 |
60 |
62.5 |
64 |
59 |
58 |
61 |
62 |
56 |
58 |
| Median Survival |
20 |
5.1 |
22 |
17 |
12 |
14 |
21 |
14 |
12 |
12 |
| (weeks) |
| Lung to Diagnosis |
7 |
7.1 |
10.2 |
12 |
15 |
11.1 |
12 |
12.2 |
17 |
16.4 |
| (month) |
| Adenocarcinoma |
24 |
32 |
42 |
67 |
97 |
135 |
85 |
83 |
101 |
30 |
| Intra-CSF |
32 |
2 |
48 |
37 |
7 |
109 |
42 |
27 |
59 |
2 |
| systemic |
20 |
20 |
22 |
37 |
20 |
29 |
59 |
51 |
53 |
21 |
| WBRT |
9 |
10 |
27 |
29 |
46 |
67 |
49 |
21 |
18 |
19 |
| WBRT Survival |
No |
No |
yes |
yes |
no |
yes |
yes |
yes |
No |
no |
| ECOG PS <=2 |
32 |
17 |
35 |
37 |
63 |
129 |
87 |
52 |
50 |
14 |
| ECOG > 2 |
|
17 |
15 |
30 |
62 |
20 |
21 |
39 |
55 |
16 |
| EGFR TKI |
0 |
0 |
14 |
37 |
9 |
24 |
42 |
51 |
29 |
21 |
Five out of ten studies reported survival benefit with WBRT. Table 7 shows the comparison of LMC patients who experienced survival benefit with WBRT.
Table 7: Analysis of factors associated with survival benefit of WBRT.
| |
WBRT with Survival Benefit |
WBRT With No Survival Benefit |
|
| (5 studies) |
(5 studies) |
P value |
| Number of Patients |
465 |
326 |
|
| Median Age |
61.5 |
60.4 |
|
| Median Survival (weeks) |
17.6 |
12.2 |
0.0412 |
| Lung to Diagnosis (month) |
14.24 |
12.5 |
0.56 |
| Adenocarcinoma |
412 (87%) |
284 (87%) |
0.94 |
| Intra-CSF |
226 (49%) |
102 (31%) |
<0.0001 |
| Systemic |
198 (43%) |
134 (41%) |
0.29 |
| WBRT |
193 (41%) |
102 (31%) |
0.0063 |
| ECOG PS <=2 |
340 (73%) |
176 (54%) |
<0.0001 |
| ECOG > 2 |
125 (26%) |
150 (46%) |
<0.0001 |
| EGFR TKI |
168 (36%) |
59 (18%) |
<0.0001 |
Statistically significant factors include IT chemotherapy, performance score, and EGFR TKI treatment. The median survival was higher among patients who benefited longer survival with WBRT (17.6 weeks vs 12.2 weeks). The performance score was substantially better for those who benefitted the longer survival with WBRT. Not surprisingly, the group with benefitted survival from WBRT had substantially higher percentage treated with EGFR-TKI (36% vs 18%). Based on such findings, a general algorithm for a patient with LMC with NSCLC who can potentially experience survival benefit from WBRT (gray box) can be created, as shown by Figure 4.

Figure 4: Algorithm for recommending RT therapy for survival benefit based on 10 studies for LMC NSCLC.
Discussion
To our knowledge, this is the first synthesized literature review analyzing factors that have statistical significance in regards to survival benefit of RT in LMC patients. Many retrospective studies have been published with different conclusions on relationship between RT and its survival benefit. Such conflicting results are not surprising given the nature of retrospective study, complex treatment regimen of LMC patients, and varying degree of prognostic factors associated with patient population in different studies. Therefore, systemic review on published studies to investigate the inconsistent conclusions on survival benefit of RT and identifying factors that lead to the discrepancy would benefit clinicians in providing optimal treatment to LMC patients.
The role of RT for LMC patients comes in two-folds. First role is to facilitate successful treatment course of IT chemotherapy by correcting CSF outflow obstruction which exists in more than 50% of LMC patients [15]. Second role is to relieve symptoms and mass effects. RT has shown survival benefit in both categories [17,31,40].
Indirect survival benefit of RT by correcting CSF outflow obstruction is reported by multiple studies [15,17,44]. In study by Glantz et al., [17], patients who started with abnormal CSF flow and corrected with RT (n =9) had longer median survival than those with normal CSF flow (n=13) with statistical significance (13 months vs 7 months). In addition to correcting obstruction, performance and extent of systemic disease involvement were reported to have contributed to longer survival compared to normal-flow patients. But in the same study, patients with CSF outflow abnormality that were not correctable with RT (n=9) had much shorter median survival compared to those corrected (13 months vs 0.7 months). Among uncorrectable population, only 2 out of 9 patients had significant performance degradation with cranial nerve involvement compared to outflow-corrected group. Otherwise, performance characteristics and systemic involvement were very similar between two groups.
Hence, there is a clear survival benefit if CSF out flow obstruction can be corrected. Therefore, it is important to emphasize how RT plays a vital role allowing IT chemotherapy to work properly which is the mainstay of LMC treatment today. Today, NCCN guideline strongly recommends CSF flow study once LMC patient is categorized into good risk group.
For LMC patients from the breast cancer, seven studies were identified that met our searching criteria. Two of seven studies concluded WBRT has survival benefit. Using survival benefit with WBRT as a variable, two groups were created. Group1 (n=185) was from two studies [31,35] that showed survival benefit and group2 (n = 207) from studies that did not show survival benefit with the WBRT. Group1 had longer median survival compared to group 2 (17.6 vs. 12.2 weeks) with statistical significance. Factors that showed statistical significance between group1 and group 2 included KPS>60, IT chemotherapy, systemic treatment, WBRT, and the severity of systemic disease including metastases to other organs.
In general, KPS score is a strong prognostic factor for all cancer treatments [45]. All seven studies reported KPS>60 to be a positive prognostic factor for overall survival regardless of the survival benefit from theWBRT. KPS score is directly related to the status of the CNS involvement and recent study showed that there is a correlation between high KPS score and survival benefit from WBRT for patients with CNS metastasis [46,47].Therefore, higher performing patients benefit more from WBRT treatment is predictable to a certain degree. Multimodality treatment (IT + RT + Systemic) was another factor. Group1 received more triple modality treatment than group2 (55% vs 33%). Multiple studies report synergistic effect when you combine multiple treatment modalities. Systemic chemotherapy and targeted therapy help eradicate disease in systemic sites that IT cannot reach due to blood brain barrier. Also, RT can provide deeper penetration into CNS tissue compared to IT whose penetration is limited to about 2-3mm [48]. Extent of metastasis to other organs also played significant role whether patients would experience survival benefit or not from the WBRT.Group1 had substantially lower systemic metastasis compared to group2 (46% vs 67%). Explanationfor such results align with KPS score. Low KPS score often correlate with more extensive systemic involvement [49]. Hence it is not surprising that factors contributed to WBRT survival benefitincluded both KPS score and severity of systemic involvement with statistical significance.
For LMC patients with NSCLC primary, ten studies were identified. Factors that showed statistical significance with WBRT survival benefit were KPS score, WBRT, IT chemotherapy, and EGFR-TKI treatment. KPS score and IT chemotherapy share the same rationale with breast cancer patients. For the past decade, use of EGFR-TKI for NSCLC whose mechanism involves activating mutations in exons 19 and 21, has shown substantial survival benefit [39,40,50]. When EGFR-TKI is combined with WBRT, synergistic effects have been reported with survival benefit for patients with NSCLC with brain metastasis [51,52]. Study from Welsh et al., [51] showed increased survival by 11.8 months when treated with EGFR-TKI with WBRT. It is believed that WBRT injures the blood brain barrier and allows better penetration and higher concentration of EGFR-TKI agents into CNS parenchyma [43,53,54].
Conclusion
The role of RT and its survival benefit for LMC patients are reviewed. Factors that are associated with WBRT survival benefit are systemically derived and extensively discussed. Though multiple factors are identified, KPS score seems to be the single most important prognostic factor that governs the survival benefit associated with WBRT. Algorithms for LMC patients with breast or lung cancer are devised. Such algorithm can serve as a general guideline to assess patient profile that can potentially have survival benefit by receiving WBRT.
References
1. Chamberlain MC. Leptomeningeal metastasis. Current opinion in oncology. 2010; 22: 627-635.
2. Groves MD. New strategies in the management of leptomeningeal metastases. Archives of neurology. 2010; 67: 305-312.
3. Shapiro WR, Posner JB, Ushio Y, Chemik NL, Young DF. Treatment of meningeal neoplasms. Cancer treatment reports. 1977; 61: 733-743.
4. Kaplan JG, DeSouza TG, Farkash A. Leptomeningeal metastases: comparison of clinical features and laboratory data of solid tumors, lymphomas and leukemias. J Neurooncol. 1990; 9: 225-229.
5. Chamberlain MC. Combined-modality treatment of leptomeningeal gliomatosis. Neurosurgery. 2003; 52: 324-329; 330.
6. Kesari S, Batchelor TT. Leptomeningeal metastases. Neurologic clinics. 2003; 21: 25-66.
7. Beauchesne P. Intrathecal chemotherapy for treatment of leptomeningeal dissemination of metastatic tumours. The Lancet Oncology. 2010; 11: 871 879.
8. Bruna J, Gonzalez L, Miro J, Velasco R, Gil M, Tortosa A. Leptomeningeal carcinomatosis: prognostic implications of clinical and cerebrospinal fluid features. Cancer. 2009; 115: 381-389.
9. Kim DY, Lee KW, Yun T. Comparison of intrathecal chemotherapy for leptomeningeal carcinomatosis of a solid tumor: methotrexate alone versus methotrexate in combination with cytosine arabinoside and hydrocortisone. Japanese journal of clinical oncology. 2003; 33: 608-612.
10. Hitchins RN, Bell DR, Woods RL, Levi JA. A prospective randomized trial of single-agent versus combination chemotherapy in meningeal carcinomatosis. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 1987; 5: 1655-1662.
11. Mehta AI, Brufsky AM, Sampson JH. Therapeutic approaches for HER2 positive brain metastases: circumventing the blood-brain barrier. Cancer Treat Rev. 2013; 39: 261-269.
12. Grossman SA, Krabak MJ. Leptomeningeal carcinomatosis. Cancer Treatment Reviews. 1999; 25: 103-119.
13. Network NCC. Central Nervous System Cancers. 2016.
14. Feyer P, Sautter-Bihl M-L, Budach W. DEGRO Practical Guidelines for Palliative Radiotherapy of Breast Cancer Patients: Brain Metastases and Leptomeningeal Carcinomatosis. Strahlentherapie und Onkologie. 2010; 186: 63-69.
15. Grossman SA, Trump DL, Chen DC, Thompson G, Camargo EE. Cerebrospinal fluid flow abnormalities in patients with neoplastic meningitis. An evaluation using 111indium-DTPA ventriculography. The American journal of medicine. 1982; 73: 641-647.
16. Scott BJ, Kesari S. Leptomeningeal metastases in breast cancer. American Journal of Cancer Research. 2013; 3: 117-126.
17. Glantz MJ, Hall WA, Cole BF. Diagnosis, management, and survival of patients with leptomeningeal cancer based on cerebrospinal fluid-flow status. Cancer. 1995; 75: 2919-2931.
18. Kiyatkin EA, Sharma HS. Acute Methamphetamine Intoxication: Brain Hyperthermia, Blood-Brain Barrier and Brain Edema. International review of neurobiology. 2009; 88: 65-100.
19. Chamberlain MC, Corey-Bloom J. Leptomeningeal metastases: 111indium DTPA CSF flow studies. Neurology. 1991; 41: 1765-1769.
20. Wasserstrom WR, Glass JP, Posner JB. Diagnosis and treatment of leptomeningeal metastases from solid tumors: experience with 90 patients. Cancer. 1982; 49: 759-772.
21. Battal B, Kocaoglu M, Bulakbasi N, Husmen G, Tuba Sanal H, Tayfun C. Cerebrospinal fluid flow imaging by using phase-contrast MR technique. The British Journal of Radiology. 2011; 84: 758-765.
22. Leal T, Chang JE, Mehta M, Robins HI. Leptomeningeal Metastasis: Challenges in Diagnosis and Treatment. Current cancer therapy reviews. 2011; 7: 319-327.
23. Chamberlain MC, Kormanik PA. Prognostic significance of 111indium-DTPA CSF flow studies in leptomeningeal metastases. Neurology. 1996; 46: 1674 1677.
24. Chamberlain MC, Sandy AD, Press GA. Leptomeningeal metastasis: a comparison of gadolinium-enhanced MR and contrast-enhanced CT of the brain. Neurology. 1990; 40: 435-438.
25. Clarke JL, Perez HR, Jacks LM, Panageas KS, Deangelis LM. Leptomeningeal metastases in the MRI era. Neurology. 2010; 74: 1449-1454.
26. Van Horn A, Chamberlain MC. Neoplastic meningitis. The journal of supportive oncology. 2012; 10: 45-53.
27. Groves MD. The pathogenesis of neoplastic meningitis. Current Oncology Reports. 2003; 5: 15-23.
28. Kokkoris CP. Leptomeningeal carcinomatosis. How does cancer reach the pia-arachnoid? Cancer. 1983; 51: 154-160.
29. Boogerd W, van den Bent MJ, Koehler PJ. The relevance of intraventricular chemotherapy for leptomeningeal metastasis in breast cancer: a randomised study. Eur J Cancer. 2004; 40: 2726-2733.
30. Grossman SA, Finkelstein DM, Ruckdeschel JC, Trump DL, Moynihan T, Ettinger DS. Randomized prospective comparison of intraventricular methotrexate and thiotepa in patients with previously untreated neoplastic meningitis. Eastern Cooperative Oncology Group. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 1993; 11: 561-569.
31. Niwińska A, Rudnicka H, Murawska M. Breast cancer leptomeningeal metastasis: propensity of breast cancer subtypes for leptomeninges and the analysis of factors influencing survival. Medical Oncology (Northwood, London, England). 2013; 30: 408.
32. Tham Y-L, Sexton K, Kramer R, Hilsenbeck S, Elledge R. Primary breast cancer phenotypes associated with propensity for central nervous system metastases. Cancer. 2006; 107: 696-704.
33. Boyle R, Thomas M, Adams JH. Diffuse involvement of the leptomeninges by tumour-a clinical and pathological study of 63 cases. Postgraduate medical journal. 1980; 56: 149-158.
34. Glantz MJ, Jaeckle KA, Chamberlain MC. A randomized controlled trial comparing intrathecal sustained-release cytarabine (DepoCyt) to intrathecal methotrexate in patients with neoplastic meningitis from solid tumors. Clinical cancer research: an official journal of the American Association for Cancer Research. 1999; 5: 3394-3402.
35. Rudnicka H, Niwinska A, Murawska M. Breast cancer leptomeningeal metastasis--the role of multimodality treatment. J Neurooncol. 2007; 84: 57-62.
36. Le Rhun E, Taillibert S, Chamberlain MC. Carcinomatous meningitis: Leptomeningeal metastases in solid tumors. Surgical Neurology International. 2013; 4: S265-S288.
37. Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA: a cancer journal for clinicians. 2011; 61: 69-90.
38. Park JH, Kim YJ, Lee JO. Clinical outcomes of leptomeningeal metastasis in patients with non-small cell lung cancer in the modern chemotherapy era. Lung cancer (Amsterdam, Netherlands). 2012; 76: 387-392.
39. Morris PG, Reiner AS, Szenberg OR. Leptomeningeal metastasis from non-small cell lung cancer: survival and the impact of whole brain radiotherapy. Journal of thoracic oncology: official publication of the International Association for the Study of Lung Cancer. 2012; 7: 382-385.
40. Lee SJ, Lee JI, Nam DH, et al. Leptomeningeal carcinomatosis in non-small-cell lung cancer patients: impact on survival and correlated prognostic factors. Journal of thoracic oncology: official publication of the International Association for the Study of Lung Cancer. 2013; 8: 185-191.
41. Kim D-Y, Lee K-W, Yun T. Comparison of Intrathecal Chemotherapy for Leptomeningeal Carcinomatosis of a Solid Tumor: Methotrexate Alone Versus Methotrexate in Combination with Cytosine Arabinoside and Hydrocortisone. Japanese journal of clinical oncology. 2003; 33: 608-612.
42. Nakamura Y, Takahashi T, Tsuya A. Prognostic Factors and Clinical Outcome of Patients with Lung Adenocarcinoma with Carcinomatous Meningitis. Anticancer Research. 2012; 32: 1811-1816.
43. Xu Q, Chen X, Qian D. Treatment and prognostic analysis of patients with leptomeningeal metastases from non-small cell lung cancer. Thoracic Cancer. 2015; 6: 407-412.
44. Chamberlain MC, Kormanik P. Carcinoma meningitis secondary to non-small cell lung cancer: combined modality therapy. Archives of neurology. 1998; 55: 506-512.
45. West H, Jin JO. Performance status in patients with cancer. JAMA Oncology. 2015; 1: 998-998.
46. Reali A, Allis S, Girardi A, Verna R, Bianco L, Redda MGR. Is Karnofsky Performance Status Correlate with Better Overall Survival in Palliative Conformal Whole Brain Radiotherapy? Our Experience. Indian Journal of Palliative Care. 2015; 21: 311-316.
47. Gallego Perez-Larraya J, Hildebrand J. Brain metastases. Handbook of clinical neurology. 2014; 121: 1143-1157.
48. Pardridge WM. Drug transport in brain via the cerebrospinal fluid. Fluids and Barriers of the CNS. 2011; 8: 7-7.
49. Chamberlain MC, Johnston SK, Glantz MJ. Neoplastic meningitis–related prognostic significance of the karnofsky performance status. Archives of neurology. 2009; 66: 74-78.
50. Porta R, Sanchez-Torres JM, Paz-Ares L. Brain metastases from lung cancer responding to erlotinib: the importance of EGFR mutation. The European respiratory journal. 2011; 37: 624-631.
51. Welsh JW, Komaki R, Amini A. Phase II trial of erlotinib plus concurrent whole-brain radiation therapy for patients with brain metastases from non-small-cell lung cancer. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 2013; 31: 895-902.
52. Liao BC, Lee JH, Lin CC. Epidermal Growth Factor Receptor Tyrosine Kinase Inhibitors for Non-Small-Cell Lung Cancer Patients with Leptomeningeal Carcinomatosis. Journal of thoracic oncology: official publication of the International Association for the Study of Lung Cancer. 2015; 10: 1754-1761.
53. d’Avella D, Cicciarello R, Angileri FF, Lucerna S, La Torre D, Tomasello F. Radiation-induced blood-brain barrier changes: pathophysiological mechanisms and clinical implications. Acta neurochirurgica. 1998; 71: 282-284.
54. d’Avella D, Cicciarello R, Albiero F. Quantitative study of blood-brain barrier permeability changes after experimental whole-brain radiation. Neurosurgery. 1992; 30: 30-34.